Chapter: Biology of Disease: Disorders of the Endocrine System
CushingŌĆÖs Syndrome - Disorders of the Adrenal Cortex
CUSHINGŌĆÖS SYNDROME
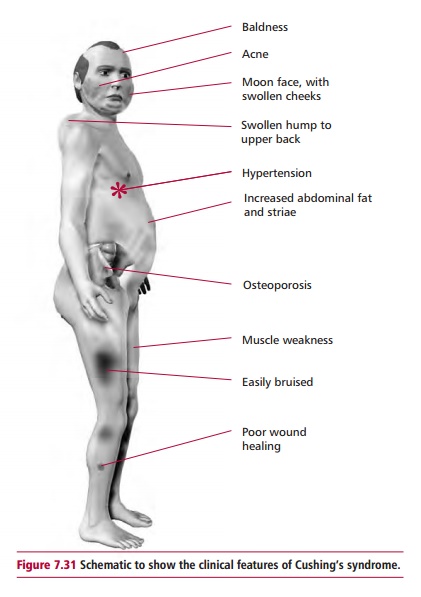
Adrenal hyperfunction can cause CushingŌĆÖs syndrome and arise from a number of causes. The commonest cause is a pituitary lesion secreting high levels of ACTH (referred to as CushingŌĆÖs disease). Other causes include ectopic production of ACTH from a carcinoma of the lungs, or excessive production of cortisol from an adrenal adenoma or carcinoma and iatrogenic causes, such as corticosteroid or ACTH treatment. The major clinical features (Figure7.31) include truncal obesity, thinning of skin, excessive bruising, poor woundhealing, purple striae on the abdomen and thighs, muscle weakness and wasting, hirsutism, the development of increased body hair on the face, chest upper back and abdomen in females (especially in adrenal carcinoma), hyper-tension, amenorrhea and psychiatric disturbances. Excess of cortisol has a mineralocorticoid effect leading to the retention of Na+ and water producing hypertension. Hypokalemia may also occur because of an excessive loss of K+ . Excess cortisol increases blood glucose levels and some of these patients may have diabetes mellitus. The clinical features are due to increased cortisol production and, partly, to excessive androgen release.
Diagnosis and treatment of CushingŌĆÖs syndrome
A clinical suspicion of the syndrome is supported by hypokalemia and alkalosis, high urinary free cortisol, which is normally less than 300 nmol per 24 h, and loss of the usual diurnal rhythm of cortisol secretion. Initial screening criteria are followed by tests using the cortisol analog, dexamethasone, which is not detected by the usual methods of measuring cortisol. Dexamethasone, however, suppresses ACTH production and cortisol secretion in normal people. The low dose dexamethasone test involves giving 1 mg of dexamethasone at night. A blood specimen is taken for cortisol measurement the following morning. A failure of dexamethasone to suppress cortisol release is suggestive of CushingŌĆÖs syndrome or disease. To distinguish between the two, a high dose dexamethasone test may be used or the concentration of ACTH in plasma measured. The high dose dexamethasone test consists of administering 2 mg of dexamethasone every 6 h for a period of 48 h. The concentration of cortisol in the plasma is then measured at 09.00 h on the morning following the last dose. In CushingŌĆÖs syndrome, due to excessive secretion of cortisol by an adrenal tumor or in response to an ectopic source of ACTH, suppression of cortisol does not occur. In CushingŌĆÖs disease, caused by a pituitary lesion secreting ACTH, the concentration of cortisol is suppressed to less than 50% of its value prior to the test. Plasma ACTH levels are raised in patients with CushingŌĆÖs disease and ectopic ACTH production, but are low in patients who have an adrenal tumor that secretes cortisol.
The management and treatment of CushingŌĆÖs syndrome depends upon its cause. Drugs, such as metyrapone, that inhibit the synthesis of cortisol may be used. Tumors can be removed surgically.
Related Topics