Chapter: Clinical Anesthesiology: Regional Anesthesia & Pain Management: Chronic Pain Management
Entrapment Syndromes
Selected Pain Syndromes
ENTRAPMENT SYNDROMES
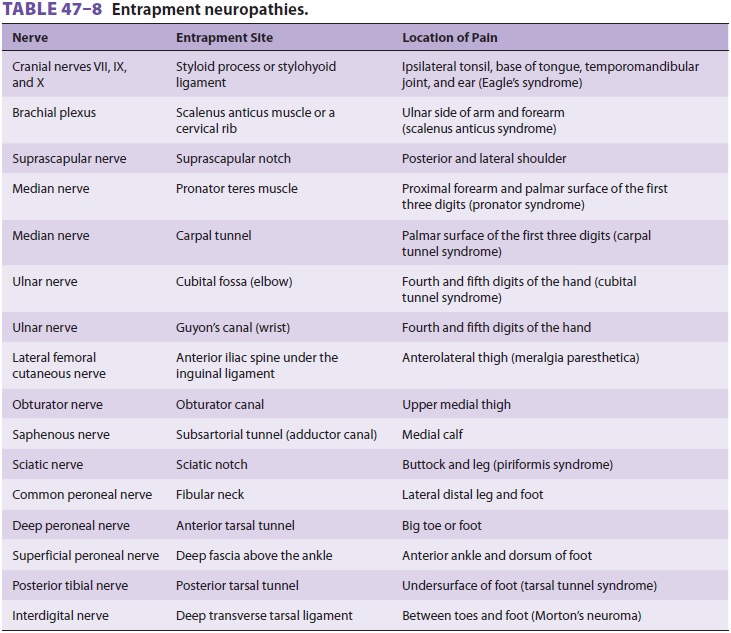
Neural compression may occur wherever a nerve courses through an
anatomically narrowed pas-sage, and entrapment neuropathies can involve
sensory, motor, or mixed nerves. Genetic factors and repetitive macrotrauma or
microtrauma are likely involved, and adjacent tenosynovitis is often
responsible. Table 47–8 lists the most commonly recognized
entrapment syndromes. When a sen-sory nerve is involved, patients complain of
pain and numbness in its distribution distal to the site of entrapment;
occasionally, a patient may complain of pain referred proximal to the site of
entrapment. Entrapment of the sciatic nerve can mimic a her-niated
intervertebral disc. Entrapment of a motor nerve produces weakness in the
muscles it inner-vates. Even entrapments of “pure” motor nerves can produce a
vague pain that may be mediated by
afferent fibers from muscles and joints. The diag-nosis can usually be
confirmed by electromyogra-phy and nerve conduction studies. Neural blockade of
the nerve with local anesthetic, with or without corticosteroid, may be
diagnostic and can provide temporary pain relief. Treatment is generally
symp-tomatic with oral analgesics and temporary immo-bilization, whenever
appropriate. Development of complex regional pain syndrome may respond to
sympathetic blocks. Refractory symptoms may require surgical decompression.
Related Topics