Chapter: Clinical Anesthesiology: Regional Anesthesia & Pain Management: Chronic Pain Management
Cancer Related Pain - Chronic Pain Management
CANCER RELATED PAIN
Cancer-related pain may be due to the
cancerous lesion itself, metastatic disease, complications such as neural
compression or infection, or treatment such as chemotherapy or radiation
therapy. In addi-tion, the cancer patient may have acute or chronic pain that
is entirely unrelated to the cancer. The pain manager must therefore have a
thorough under-standing of the nature of the cancer, its stage, the presence of
metastatic disease, and treatments.
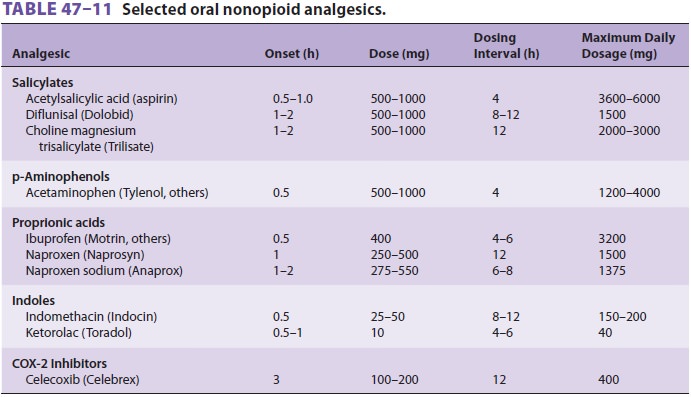
Cancer pain can be managed with oral
analge-sics in most patients. The World Health Organization recommends a
progressive, three-step approach: (1) nonopioid analgesics such as aspirin,
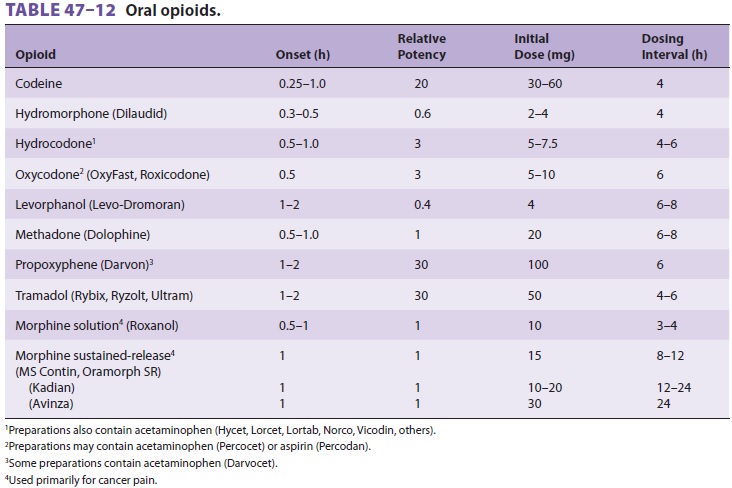
acetamino-phen, or NSAID for mild pain, (2) “weak” oral opi-oids (codeine and
oxycodone) for moderate pain, and (3) stronger opioids (morphine and
hydromor-phone) for severe pain (Tables 47–11
and 47–12). Parenteral therapy is necessary when
patients have refractory pain, cannot take medication orally, or have poor
enteral absorption. Regardless of the agent selected, in most instances drug
therapy should be provided on a fixed time schedule rather than as needed.
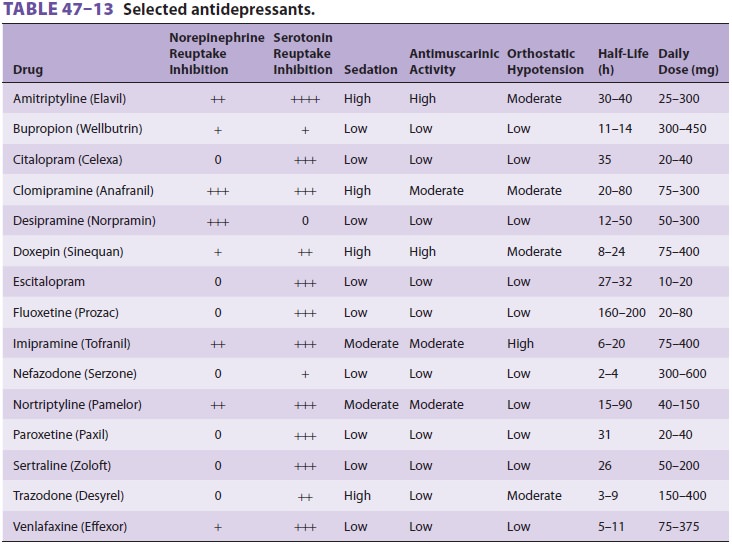
Adjuvant drug therapy, particularly antidepressants, and other modalities
should also be used liberally in patients with cancer-related pain (Table
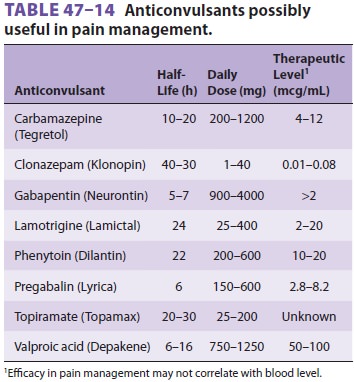
47–13). Anticonvulsants may be use-ful (Table
47–14). Intrathecal drug delivery sys-tems may
improve analgesia and, via a drug-sparing effect, help decrease side effects
associated with oral or intravenous agents. Numerous intrathecal agents have
been studied, and opioids have been utilized both alone and in combination with
other medica-tions. Ziconotide is a direct-acting N-type calcium-channel
blocker that may be helpful for refractory pain or as a first-line agent. It
acts by decreasing the release of substance P from the presynaptic nerve
terminal in the dorsal horn of the spinal cord. Side effects may be dose dependent
and include audi-tory hallucinations and worsening of depression or psychosis.
It does not lead to significant withdrawal conditions if abruptly discontinued.
Surgery, radiation therapy, and chemotherapy may prolong survivorship for patients with cancer. However, survivorship may be accompanied by therapy-related acute or chronic pain, including radiation fibrosis or chemotherapy-induced periph-eral neuropathy. Treatment of these pain conditions is an area of ongoing research.
Related Topics