Chapter: Ophthalmology: The Eyelids
Ptosis
Ptosis
Definition
Paralysis of the levator palpebrae muscle with
resulting drooping of one or both upper eyelids (from the Greek ptosis, a falling). The following forms
are differentiated according to their origin (see also Etiology):
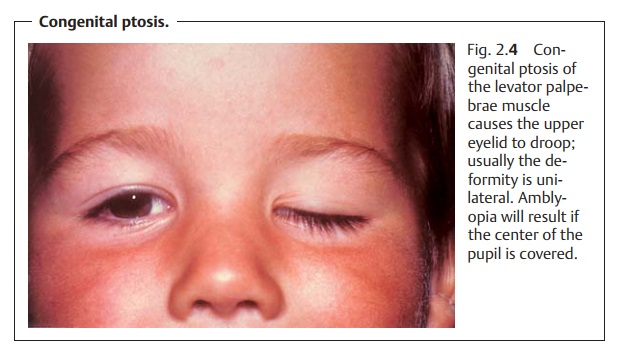
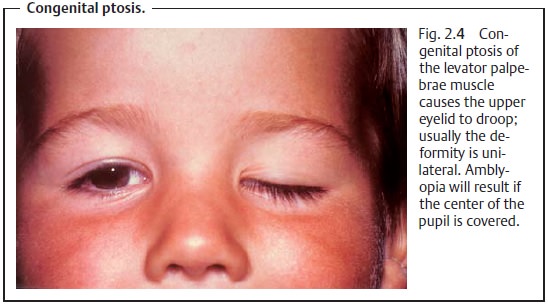
❖Congenital ptosis (Fig. 2.4).
❖ Acquired ptosis:
–
Paralytic ptosis.
–
Sympathetic ptosis.
–
Myotonic ptosis.
–
Traumatic ptosis.
Epidemiology.On the whole ptosis is a rare disorder.
Etiology: Ptosis may be congenital or acquired.
Congenital ptosis.The disorder is usually hereditary and is primarily auto-somal
dominant as opposed to recessive. The cause is frequently aplasia in the core of the oculomotor
nerve (neurogenic) that supplies the levator palpe-brae muscle; less
frequently it is attributable to an underdeveloped
levatorpalpebrae muscle (myogenic).
Acquired ptosis:
❖ Neurogenic causes:
–
Oculomotor palsy (paralytic ptosis).
– Lesions in the sympathetic nerve (sympathetic ptosis) is Horner’s palsy
(ptosis, miosis, and enophthalmos).
❖Myogenic ptosis: myasthenia gravis and myotonic
dystrophy.
❖ Traumatic ptosis can occur after injuries.
Symptoms.The drooping of the upper eyelid may beunilateral(usually a signof a neurogenic
cause) or bilateral (usually a sign
of a myogenic cause). A
characteristic feature of the unilateral
form is that the patient attempts to increase the palpebral fissure by
frowning (contracting the frontalis muscle). Congenital ptosis (Fig. 2.4)
generally affects one eye only; bilateral symptomsare observed far less
frequently (7%).
Diagnostic considerations: Congenital ptosis.The affected eyelid in generalis
underdeveloped. The skin of the upper eyelid is smooth and thin; the supe-rior
palpebral furrow is absent or ill-defined. A typical symptom is “lid lag” in which the upper eyelid does
not move when the patient glances down. Thisimportant
distinguishing symptom excludes acquired ptosis in differential diag-nosis. In
about 3% of all cases, congenital ptosis is associated with epicanthalfolds and
blepharophimosis (Waardenburg syndrome).
Congenital ptosis can occur in varying degrees
of severity and may be com-plicated by the presence of additional eyelid and
ocular muscle disorders such as strabismus.
Congenital ptosis in which the upper eyelid
droops over the center of the pupil always involves an increased risk of
amblyopia.
Acquired ptosis:
❖ Paralytic ptosis in oculomotor palsy is usually unilateralwith the drooping
eyelid covering the whole eye. Often there will be other signs of palsy in the
area supplied by the oculomotor nerve. In externaloculomotor
palsy, only the extraocular muscles are affected (mydriasis willnot be
present), whereas in complete oculomotor
palsy, the inner ciliary muscle and the sphincter pupillae muscle are also
affected (internal oph-thalmoplegia with loss of accommodation, mydriasis, and
complete loss of pupillary light reflexes).
❖ Myasthenia gravis (myogenic ptosis that is often bilateral and
may beasymmetrical) is associated with abnormal fatigue of the
striatedvextraocular muscles. Ptosis typically becomes more severe as the day
goes on.
❖ Sympathetic ptosis occurs in Horner’s palsy (ptosis, miosis, and enophthal-mos).
Rapidly opening and closing the eyelids
provokes ptosis in myasthenia gravis and simplifies the diagnosis.
Treatment:
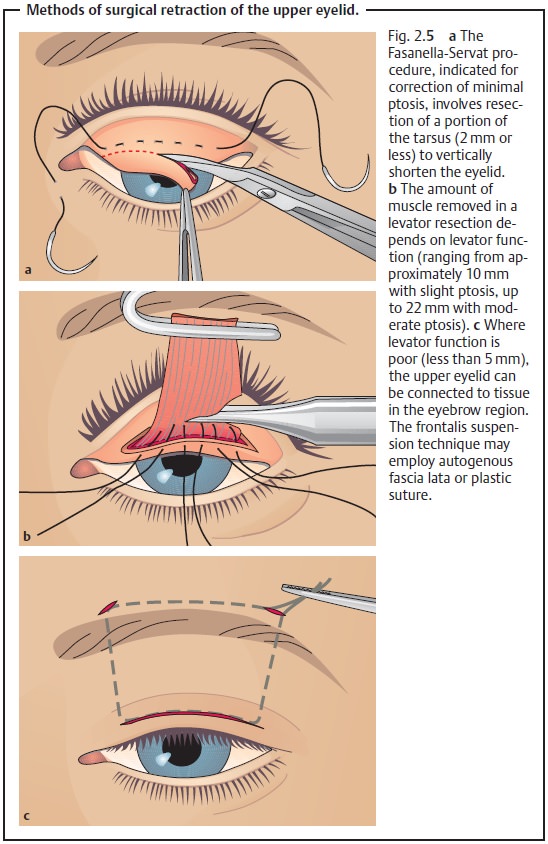
❖ Congenital ptosis: This involves surgical retraction of the upper eyelid(Fig. 2.5a – c), which should be undertaken as
quickly as possible when there is a risk of the affected eye developing a
visual impairment as a result of the ptosis.
❖ Acquired ptosis: Treatment depends on the cause. As palsies oftenresolvespontaneously, the patient should
be observed before resorting to surgica
intervention. Conservative treatment with
special eyeglasses may be suffi-cient even in irreversible cases.
Because of the risk of overcorrecting or
undercorrecting the disorder, several operations may be necessary.
Prognosis and complications: Prompt surgical intervention in congenitalptosis can prevent amblyopia. Surgical overcorrection of
the ptosis can lead to desiccation of the conjunctiva and cornea with ulceration as a result of incomplete
closure of the eyelids.
Related Topics