Chapter: Ophthalmology: The Eyelids
Eyelids: Malignant Tumors
Malignant Tumors
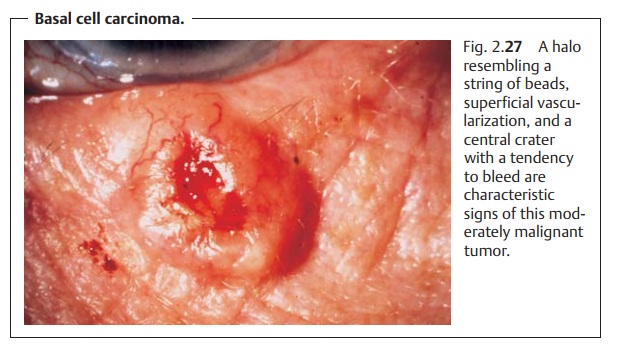
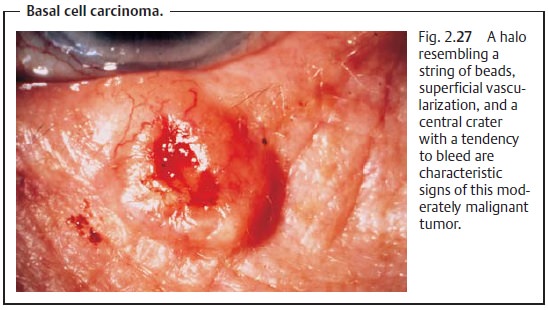
Basal Cell Carcinoma
Definition
Basal cell carcinoma is a frequent, moderately
malignant, fibroepithelial tumor that can cause severe local tissue destruction
but very rarely metastasizes.
Epidemiology:
Approximately 90% of all malignant eyelid
tumors are basalcell carcinomas. Their incidence increases with age. In
approximately 60% of all cases they are localized on the lower eyelid. Morbidity in sunny countries is 110 cases per 100000
persons (in central Europe approximately 20 per 100000 persons). Dark-skinned people are affected significantly less often.
Gender is not a predisposing factor.
Etiology:
Causes of basal cell carcinoma may include a
genetic disposition.Increased exposure to
the sun’s ultraviolet radiation, carcinogenic substances (such as arsenic),
and chronic skin damage can also lead
to an increased inci-dence. Basal cell carcinomas arise from the basal cell
layers of the epidermis and the sebaceous gland hair follicles, where their
growth locally destroys tissue.
Symptoms:
Typical characteristics include a firm,
slightly raised margin (ahalo resembling
a string of beads) with a central
crater and superficial
vascular-ization with an increased tendency to bleed (Fig. 2.27).
Ulceration with “gnawing” peripheral
proliferation is occasionally referred to as an ulcus rodens; an ulcus
terebans refers to deep infiltration with invasion of cartilage and bone.
Diagnostic considerations:
The diagnosis can very often be made on
thebasis of clinical evidence. A biopsy is indicated if there is any doubt.
Loss of the eyelashes in the vicinity of the
tumor always suggests malig-nancy.
Treatment:
The lesion is treated by surgical excision within a margin ofhealthy tissue. This is the safest method. If a radical procedure is not feasible, the only remaining options are radiation therapy or cryotherapy with liquid nitrogen.
Prognosis:
The changes of successful treatment by surgical
excision are verygood. Frequent follow-up examinations are indicated.
The earlier a basal cell carcinoma is
detected, the easier it is to remove.
Squamous Cell Carcinoma
This is the second most frequently encountered malignant eyelid tumor. The carcinoma
arises from the epidermis, grows rapidly and destroys tissue. It can
metastasize into the regional lymph nodes. Remote metastases are rarer. The treatment of choice is complete surgical
removal.
Adenocarcinoma
The rare
adenocarcinoma arises from the meibomian glands or the glands of Zeis. The firm, painless swelling is usually located in the upper eyelid and is mobile with respect to the skin but
not with respect to the underlying tissue. In its early stages it can be mistaken easily for a chalazion. The
lesion can metastasize into local lymph nodes.
An apparent chalazion that cannot be removed
by the usual surgical procedure always suggests a suspected adenocarcinoma.
The treatment
of choice is complete surgical removal.
Related Topics