Chapter: Clinical Dermatology: Infections
Molluscum contagiosum
Molluscum
contagiosum
Cause
This
common pox virus infection can be spread by direct contact; e.g. sexually or by
sharing a towel at the swimming bath.
Presentation and course
The
incubation period ranges from 2 to 6 weeks. Often several members of one family
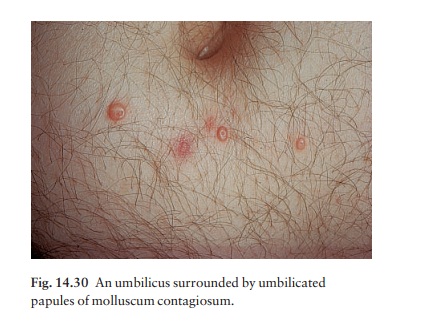
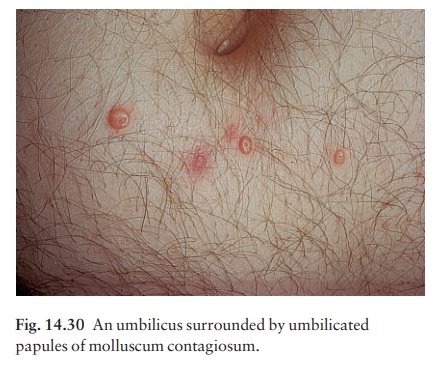
are affected. Individual lesions are shiny, white or pink, and hemi-spherical;
they grow slowly up to 0.5 cm in diameter. A central punctum, which may contain
a cheesy core, gives the lesions their characteristic umbilicated look.
On close inspection a mosaic appearance may be seen. Multiple lesions are common (Fig. 14.30) and their distribution depends on the mode of infection. Atopic individuals and the immunocompromised are prone to especially extensive infections, spread by scratching and the use of topical steroids.
Untreated
lesions usually clear in 6–9 months, often after a brief local inflammation.
Large solitary lesions may take longer. Some leave depressed scars.
Complications
Eczematous
patches often appear around mollusca. Traumatized or overtreated lesions may
become secondarily infected.
Differential diagnosis
Inflamed
lesions can simulate a boil. Large solitary lesions in adults can be confused
with a keratocan-thoma, an intradermal naevus, or even a cystic basal cell
carcinoma. Confusion with warts should not arise as these have a rough surface
and no central pore.
Investigations
None
are usually needed, but the diagnosis can be confirmed by looking under the
microscope for large swollen epidermal cells, easily seen in unstained
pre-parations of debris expressed from a lesion.
Treatment
Many
simple destructive measures cause inflamma-tion and then resolution. They
include squeezing out the lesions with forceps, piercing them with an orange
stick (preferably without phenol), and curettage. Liquid nitrogen may also be
helpful.
These
measures are fine for adults, but young children dislike them and it is
reasonable to play for time using imiquimod or chlortetracycline cream, or
instructing the mother carefully how to apply a wart paint once a week to
lesions well away from the eyes. Sometimes a local anaesthetic cream (EMLA;),
under polythene occlusion for an hour, will help children to tolerate more
attacking treatment. Sparse eyelid lesions can be left alone but patients with
numerous lesions may need to be referred to an ophthalmologist for curettage.
Common sense measures help to limit spread within the family.
Related Topics