Chapter: Basic & Clinical Pharmacology : The Gonadal Hormones & Inhibitors
Preparations & Dosages - The Estrogens
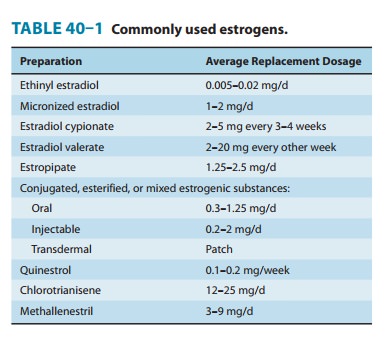
Preparations & Dosages
The dosages of
commonly used natural and synthetic preparations are listed in Table 40–1.
Although all of the estrogens produce almost the same hormonal effects, their
potencies vary both between agents and depending on the route of
administration. As noted above, estradiol is the most active endogenous
estrogen, and it has the highest affinity for the estrogen receptor. However,
its metabolites estrone and estriol have weak uterine effects.
For a given level of
gonadotropin suppression, oral estrogen preparations have more effect on the
circulating levels of CBG, SHBG, and a host of other liver proteins, including
angiotensino-gen, than do transdermal preparations. The oral route of
adminis-tration allows greater concentrations of hormone to reach the liver,
thus increasing the synthesis of these proteins. Transdermal preparations were
developed to avoid this effect. When adminis-tered transdermally, 50–100 mcg of
estradiol has effects similar to those of 0.625–1.25 mg of conjugated oral
estrogens on gonado-tropin concentrations, endometrium, and vaginal epithelium.
Furthermore, the transdermal estrogen preparations do not sig-nificantly
increase the concentrations of renin substrate, CBG, and TBG and do not produce
the characteristic changes in serum lipids. Combined oral preparations
containing 0.625 mg of con-jugated estrogens and 2.5 mg of medroxyprogesterone
acetate are available for menopausal replacement therapy. Tablets containing
0.625 mg of conjugated estrogens and 5 mg of medroxyprogester-one acetate are
available to be used in conjunction with conju-gated estrogens in a sequential
fashion. Estrogens alone are taken on days 1–14 and the combination on days
15–28.
Related Topics