Chapter: Medicine Study Notes : Cardiovascular
Physiology and Anatomy - Cardiovascular
Physiology and Anatomy
Physiology
·
Cardiac Output (CO):
o CO = MAP/TPR (ie flow = pressure / resistance)
o CO = SV * HR
o Normal adult at rest = 5 L/min
o Can be measured with Doppler/echo
·
Mean Arterial Pressure:
o MAP = Cardiac Output*TPR
o MAP = Diastolic + 1/3(systolic-diastolic)
·
Stroke volume:
o SV = End diastolic volume – end systolic volume
o Normal 60 – 80 ml
·
Ejection fraction = ESV/EDV. Determined by:
o Preload (=EDV): dependent on blood volume, venous tone, posture,
intrathoracic pressure, peripheral muscle pump, and atrial contraction (20% of
filling). Affects stroke volume through Starling‟s Law: myocardial
fibre length (ie filling) ® SV until ventricle is over-stretched. Can be measured for the left
ventricle using pulmonary artery/capillary wedge pressure (CAWP) and for the
right using central venous pressure
o Force of Contraction (Inotropy): Shifts Starling Curve up and to the
left. Increased by sympathetic stimulation, Ca, thyroxine,
angiotensin, drugs, temp, HR. Decreased by acidosis, hypoxaemia, K, drugs
(general anaesthetics, beta blockers)
o Afterload = tension in the ventricular wall at the end of systole.
Results from ventricular distension, elasticity of arterial walls and arterial
network resistance. Measure with arterial catheter
o Changes given certain shock states:

·
Peripheral vascular resistance:
o Resistance proportional to radius to the power of 4
o = (Mean aortic pressure – right atrial pressure)/cardiac output
Cardiac Anatomy
·
Heart Valves:
o Mitral valve (left AV): anterior and posterior leaflets
o Tricuspid valve: anterior,
posterior and septal cusps
o Aortic valve: left, right and posterior cusps
o Pulmonary valve: left, right and anterior cusps
·
Blood supply:
o Left main stem (LMS) ® LAD (anterior wall of LV and anterior 2/3 of septum) and Circumflex
(lateral wall of left ventricle and most of the posterior wall of the LV). Also
supplies AV node, and SA node in 60%
o Right coronary artery ® right atrium, right ventricle (except for left part of anterior wall),
right posterior and inferior walls of LV and posterior 1/3rd of septum
·
Pericardial effusion: normal
content of pericardial sac = 50 ml. Effusion can be serous, chylous or
haemorrhagic. Sign of pericarditis but also accompanies MI
Regional Blood Flow
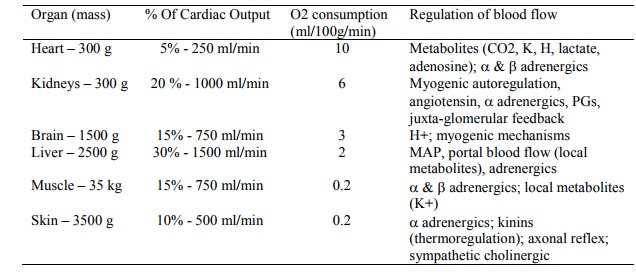
·
Cerebral Perfusion:
o Cerebral blood flow (CBF) = [MAP – ICP (or CVP, whichever is
greatest)]/cerebral vascular resistance
o Minimal desirable perfusion pressure is 60 mmHg. This is reduced by ¯arterial
pressure, venous pressure, constriction/spasm of cerebral vessels or intra-cranial
pressure (ICP)
o Autoregulation keeps CBF at 50 ml/100g/min. Less than 15 ® changes
in electrical activity
·
Coronary Perfusion:
o Perfused during diastole
o Coronary perfusion = (Mean diastolic pressure – VEDP)/Coronary Vascular
Resistance
o So treat poor perfusion with:
§ High diastolic pressure (eg systemic vasoconstrictor - a agonist)
§ Reducing end diastolic ventricular volume (prevent volume overload)
§ Decrease coronary vascular resistance (eg coronary vasodilator)
§ Slow heart rate ® longer diastolic phase (eg beta blockers)
§ ¯Preload
(nitrates and Ca channel blocker)
§ O2 therapy and maintain haemoglobin
·
Renal Perfusion:
o Normally autoregulated down to 80 mmHg systolic. When BP ¯, renal
blood flow ¯¯ ® renal failure and acute tubular necrosis
o Treatment:
§ Colloid/saline ® BP
§ Dopamine 2 – 5 mg/kg/min ® ¯renal vascular resistance
Related Topics