Chapter: Medicine Study Notes : Cardiovascular
Chest X-ray
Chest X-ray
·
First check:
o Is it the right patient
o Is it the right date
o Is it the right way round (ie L and R)
·
Then ask what is their age (and
therefore likely pathologies)
·
How was the film taken:
o Normal is PA erect, inspiratory:
§ PA as all Xray sensitive tissues are on the front (breasts, eyes,
gonads, thyroid) – less exposure
§ Scapula off chest (in an AP then scapula projected onto chest)
o Differences in Supine film:
§ Air collects on front of chest not top (important for pneumothorax)
§ Fluid distributes over back of pleura not in costophrenic angles
§ Normally more blood flow in lower zones, but in supine equal vascular
markings at top
§ Better venous return in supine ® distended great vessels
§ To tell if it‟s supine where is gastric bubble: fundus = erect, body =
supine
·
Is the film good enough:
o Is it rotated: medial ends of clavicle equidistant from spinous process
o Is it a good exposure: can you see lung veins in periphery – if you can
see the spine clearly then over exposed
o Good inspiration: 5 – 7 anterior ribs on the right (hemidiaphragm is
higher – must take a bigger breath to get it down) or 9 – 11 posterior ribs
·
Key questions:
o Is there any area that is lighter (opacity)
o Is there any area that is darker (lucency)
o Is there any abnormality of normally seen anatomy
·
Normally seen
anatomy/silhouettes:
o Right Upper quadrant (above the right bronchi):
§ SVC: free edge abutting lung
§ Right paratracheal strip (lung abutting right side of trachea). If strip
wider than 5 mm then lymph node enlargement
§ Arch of azygous in tracheal bronchial angle, just above carina. If
enlarged think RH failure or IVC obstruction
o Left Upper Quadrant (above the left bronchi):
§ Arch of aorta (aortic knuckle) and free edge of descending aorta behind
heart
§ Pulmonary trunk
§ Between them is the aortic pulmonary window: should be concave, if
convex then lymph node enlargement
o Right lower quadrant (below right bronchi): Right atrium forming the
border of the heart
o Left lower quadrant (below left bronchi):
§ Border of heart = left ventricle + left auricle of atrium (NB its below
the bronchi – a bulge above the bronchi must be something else)
§ Left hemidiaphragm (lower than the right)
o Lateral view:
§ Spine should get blacker as you go down
§ Retrosternal and retrocardiac areas should be the same density
§ Left hemi-diaphragm is the one that the heart sits on
·
Heart size:
o Enlargement: greatest transverse diameter = largest horizontal distance
from midline to right border + largest horizontal distance from midline to left
border. If this is > 50% of greatest internal diameter then the heart is
enlarged
o Signs of left atrial enlargement:
§ 2nd heart border parallel and medial to RH border (atrium bulging around
behind the RA)
§ Density
medial to this 2nd border
§ A prominent left atrial appendage
§ Elevation of the left main bronchus
o Right atrial enlargement: bulges into right lung and elevation of right
main bronchus
o Right ventricle enlargement: Apex tilts upwards. On the lateral film, area of
contact between the heart and the sternum
o Left ventricle enlargement: Elongates along its long axis ® apex
shifts down and out. Posterior bulge on the lateral film
o Causes of global heart enlargement:
§ Sack like dilatation: due to pericardial effusion, cardiomyopathy or
multi-valvular disease
§ Multi-valvular disease
§ Hypertrophic cardiomyopathy
§ Pericardial effusion
·
Progression of pulmonary oedema:
o Prominence
of upper zone vessels due to redistribution of blood to upper zones
o Leakage ® interstitial changes: peribronchial cuffing, Kerley B lines, effusion
o Flooding of the airspaces ® „Bats wing‟ appearance
o With treatment, resolves in the reverse order
·
Ribs
o Posterior of rib connects with midline, anterior doesn‟t as it turns to
cartilage which isn‟t calcified
o (but maybe in old person)
o If 1st and 2nd ribs fractured, this takes massive force, consider concurrent damage to
great vessels
o If sternum fractured, consider cardiac contusion – do cardiac enzymes
o If 11th and 12th ribs fractured, consider damage to kidney‟s, liver, spleen
o If multiple fractures: flaccid chest ® Paradoxical Breathing (segment
of chest moves in on inspiration)
·
Lobes:
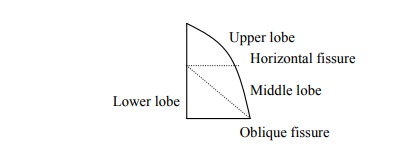
o Upper: apical, posterior, anterior
o Medial: superior, inferior
o Lower lobe: Anterior, posterior, lateral, medial, apical
·
Pathology to look out for:
o Pulmonary contusion: Opacity in parenchyma = bleeding. Should clear in 3
– 6 days (cf consolidation which may take 6 weeks to clear). May resolve
leaving clots filling cavities created from shearing forces
o Pneumothorax: must see visceral pleural edge AND no vascular markings
lateral to this edge. Edge alone might be other things
o ARDS: soft and fluffy over all the lung parenchyma
o Aspiration: won‟t be symmetrical. If it‟s global is it the „bats wing‟
appearance of pulmonary oedema?
o Is it effusion or pneumonia: Pleura is 2 cells thick. If pleural cavity
fills up loose sharp edge. If unsure, take another film lying on side (De
Cubitus view) and see if fluid level shifts. If the opacity is heterogeneous
(eg polka-dots) then pneumonia, if homogenous (a smear) then effusion
o Miliary pattern: occurs in Tb, fungi, Thyroid cancer, pneumoconiosis, rarely Sarcoid
o Cysts Þ cystic bronchiectasis.
Especially in Cystic Fibrosis and Staph.
o Enlarged hilum can be:
§ Enlarged vessels
§ Lymph node enlargement (like bunches of grapes): sarcoid, Tb, lymphoma
§ Cancer – usually unilateral
·
Differential if CXR is normal:
o Airflow obstruction: asthma, COPD
o PE
o Pneumothorax (look again…)
o Hidden pneumonia: check apices, angles and behind both sides of the
heart (can you see the diaphragm below the heart or the ribs behind the heart?)
·
Chest X ray checklist:
o A – airway – midline
o B – bones and soft tissue. Check
for gaps in bones ® ?bony metastasesC – cardiac size and silhouette. Should be < 50% of maximal internal chest
width
o D – diaphragm – right higher than left, angles sharp, contract with lung
sharp
o E – equal volume, density symmetrical
o F – fine detail (pleura & lung parenchyma)
§ Is upper darker than lower
§ Pronounced/wider vessels in upper lobes Þ
pulmonary venous congestion
§ Interstitial/pulmonary oedema ® fine diffuse shadowing
§ Kerley B lines Þ oedematous interlobular septa
§ Fluff extending from hilum (bat‟s wing appearance): alveolar pulmonary
oedema
§ Atelectesis: dense, short, usually peripheral horizontal lines. If large then collapsed lung
§ Are L & R main bronchus < 75 degrees at carina
§ If there are dots, are they hollow (if so then likely to be blood
vessels end on)
o G – gastric bubble
o H – hilum – left higher than right, no larger than thumb + Hardware
·
Don‟t make pathological diagnoses
– say an opacity consistent with
consolidation
Treat the patient not the x-ray
Related Topics