Chapter: Clinical Anesthesiology: Regional Anesthesia & Pain Management: Peripheral Nerve Blocks
Lower Extremity Peripheral Nerve Blocks: Femoral Nerve Block
Femoral Nerve Block
The femoral nerve innervates the main hip flexors, knee extensors, and
provides much of the sensory
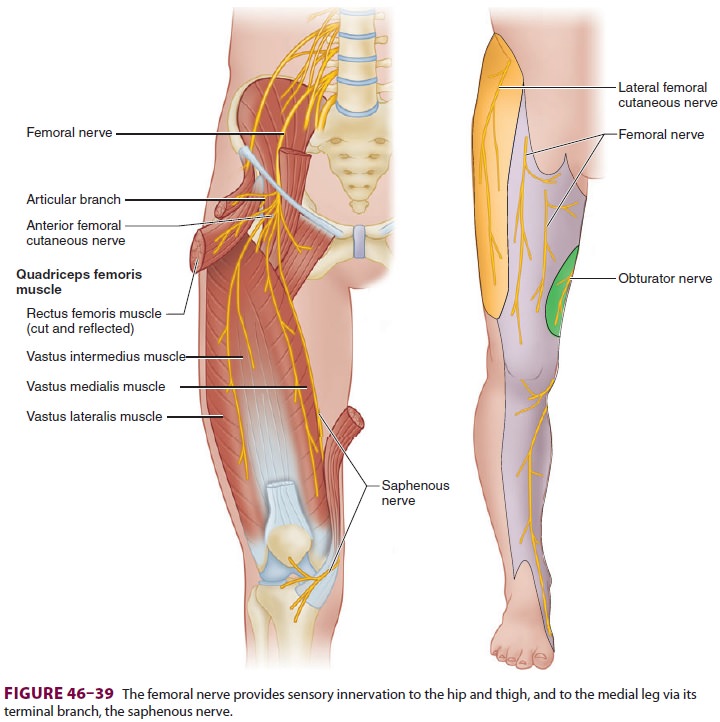
innervation of the hip and thigh (Figure
46–39). Its most medial branch is the saphenous
nerve, which innervates much of the skin of the medial leg and ankle joint. The
term 3-in-1 block refers to
anesthe-tizing the femoral, lateral femoral cutaneous, and obturator nerves
with a single injection below the inguinal ligament; this term has largely been
aban-doned as evidence accumulated demonstrating the failure of most single
injections to consistently affect
all three nerves. A femoral nerve block alone will seldom provide surgical anesthesia, but itis often used to provide postoperative analgesia for hip, thigh, knee, and ankle (for the saphenous nerve) procedures. Femoral nerve blocks have a relatively low rate of complications and few contraindications. Local infection, previous vascular grafting, and local adenopathy should be carefully considered in patient selection.
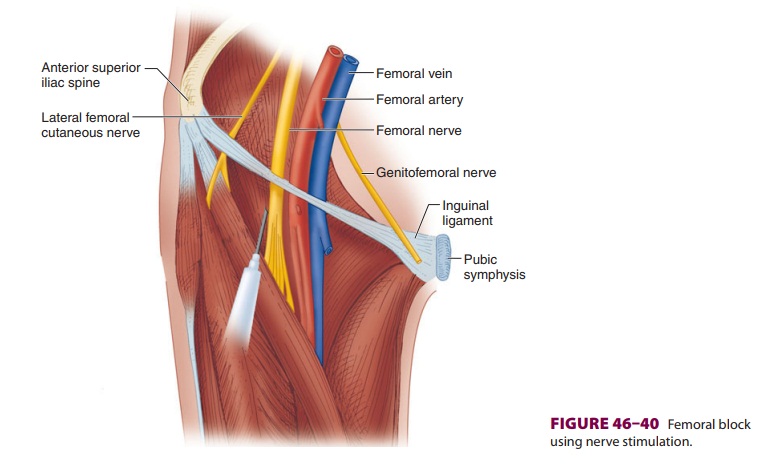
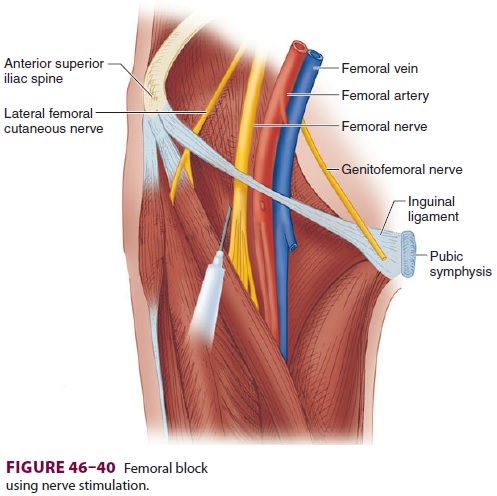
A. Nerve Stimulation
With the patient positioned supine, the
femoral artery pulse is palpated at the level of the inguinal ligament. A short
(5-cm) insulated needle is inserted at a 45° angle to the skin in a cephalad
direction (Figure 46–40) until a clear
quadriceps twitch is elicited at a current below 0.5 mA (look for patella
motion).
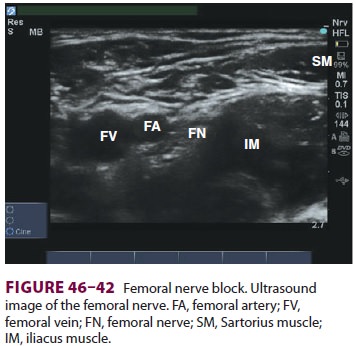
B. Ultrasound
A high-frequency linear ultrasound transducer
is placed over the area of the inguinal crease paral-lel to the crease itself,
or slightly more transverse (Figure 46–41).
The femoral artery and femoral vein are visualized in cross-section, with the
overly-ing fascia iliaca. Just lateral to the artery and deep to the fascia
iliaca, the femoral nerve appears in cross-section as a spindle-shaped
structure with a “honey-comb” texture (Figure 46–42).
For an out-of-plane technique, the block
needle is inserted just lateral to where the femoral nerve is seen, and
directed cephalad at an angle approxi-mately 45° to the skin. The needle is
advanced until it is seen penetrating the fascia iliaca, or (if using
concurrent electrical stimulation) until a motor response is elicited.
Following careful aspiration for the nonappearance of blood, 30–40 mL of local
anesthetic is injected.
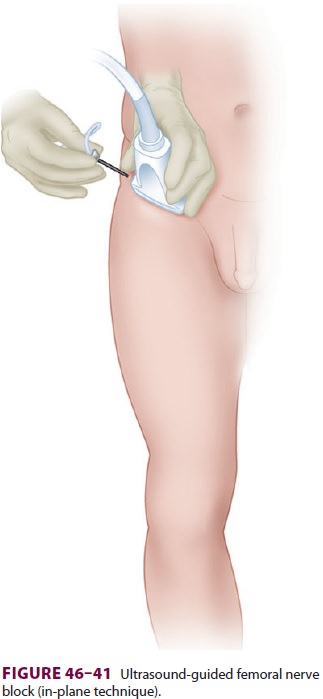
For an in-plane technique, a longer needle may be used. The needle is
inserted parallel to the ultra-sound transducer just lateral to the outer edge.
The needle is advanced through the sartorius muscle, deep to the fascia iliaca,
until it is visualized just lat-eral to the femoral nerve. Local anesthetic is
injected, visualizing its hypoechoic spread deep to the fascia iliaca and
around the nerve.
C. Fascia Iliaca Technique
The goal of a fascia iliaca block is similar to that of a femoral nerve
block, but the approach is slightly different. Without use of a nerve
stimulator or ultrasound machine, a relatively reliable level of anesthesia may
be attained simply with anatomic landmarks and tactile sensation. Once the
inguinal ligament and femoral artery pulse are identified,
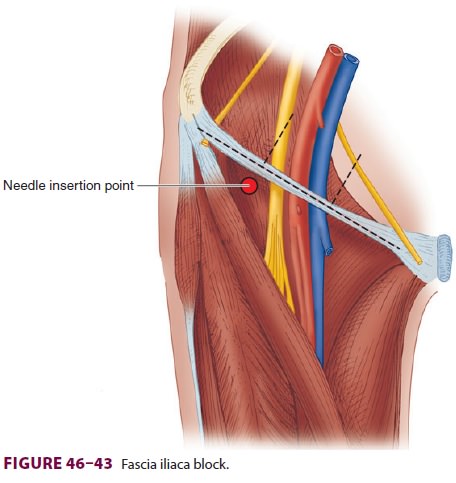
the length of the inguinal ligament is divided into thirds (Figure 46–43). Two centimeters distal to the junction of the middle and outer thirds, a short, blunt-tipped needle is inserted in a slightly cephalad direction. As the needle passes through the two layers of fascia in this region (fascia lata and fascia iliaca), two “pops” will be felt. Once the needle has passed through the fascia iliaca, careful aspiration is per-formed and 30–40 mL of local anesthetic is injected. This block usually anesthetizes both the femoral nerve and lateral femoral cutaneous nerves, since the local anesthetic is deposited under the fascia iliaca between the two nerves which run in the same plane between the fascia and underlying muscle.
Related Topics