Chapter: Clinical Anesthesiology: Regional Anesthesia & Pain Management: Peripheral Nerve Blocks
Lower Extremity Peripheral Nerve Blocks: Ankle Block
Ankle Block
For surgical procedures of the foot, an ankle block is a fast,
low-technology, low-risk means of provid-ing anesthesia. Excessive injectate
volume and use of vasoconstrictors such as epinephrine must be avoided to
minimize the risk of ischemic complica-tions. Since this block includes five
separate injec-tions, it is often uncomfortable for patients and adequate
premedication is required.
Five nerves supply sensation to the foot (Figure
46–57). The saphenous nerve is a terminal branch
of the femoral nerve and the only innervation
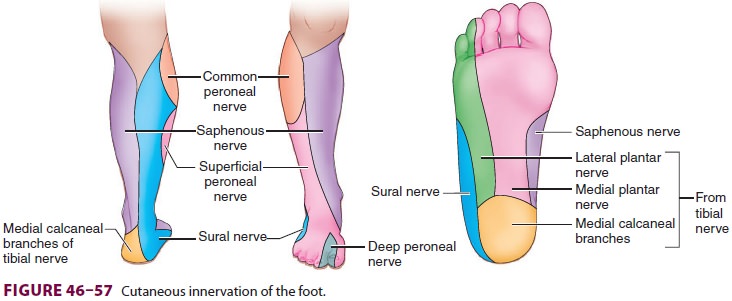
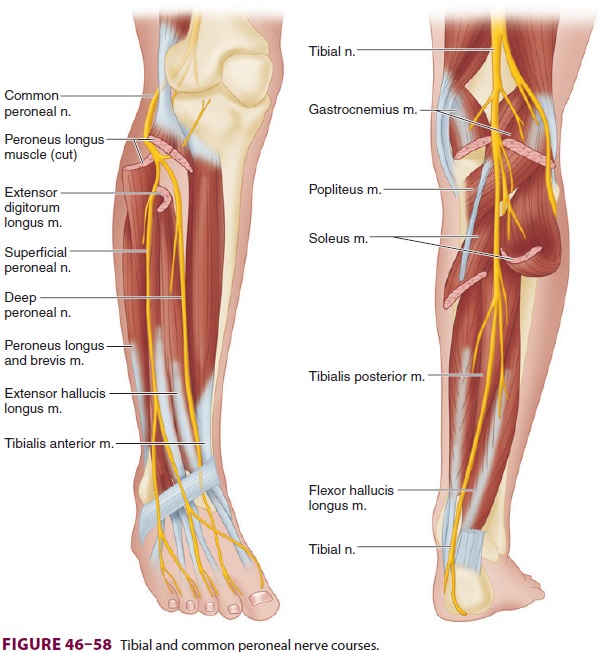
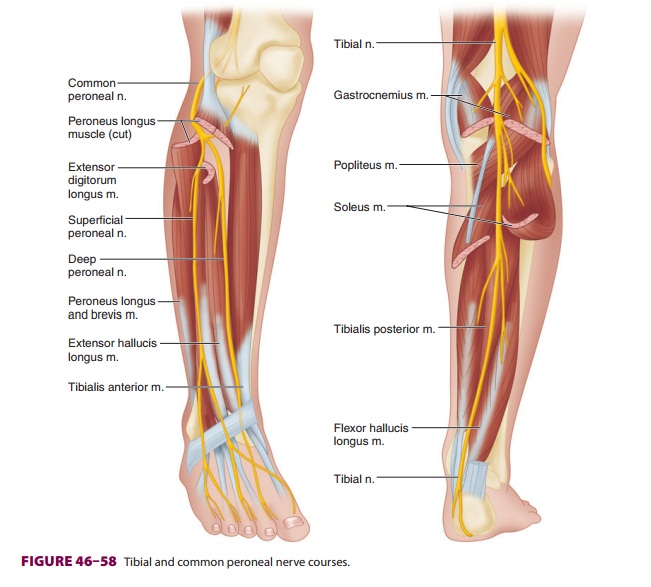
of the foot not a part of the sciatic system. It supplies superficial sensation to the anteromedial foot and is most constantly located just anterior to the medial malleolus. The deep peroneal nerve runs in the anterior leg after branching off the common pero-neal nerve, entering the ankle between the extensor hallucis longus and the extensor digitorum longus tendons (Figure 46–58), just lateral to the dorsa-lis pedis artery. It provides innervation to the toe extensors and sensation to the first dorsal webspace. The superficial peroneal nerve, also a branch of the common peroneal nerve, descends toward the ankle in the lateral compartment, giving motor branches to the muscles of eversion. It enters the ankle just lateral to the extensor digitorum longus and pro-vides cutaneous sensation to the dorsum of the foot and toes. The posterior tibial nerve is a direct continuation of the tibial nerve and enters the foot posterior to the medial malleolus, branching into calcaneal, lateral plantar, and medial plantar nerves. It is located behind the posterior tibial artery at the level of the medial malleolus and provides sensory innervation to the heel, the medial sole, and part of the lateral sole of the foot, as well as the tips of the toes. The sural nerve is a branch of the tibial nerve and enters the foot between the Achilles tendon and the lateral malleolus to provide sensation to the lateral foot.
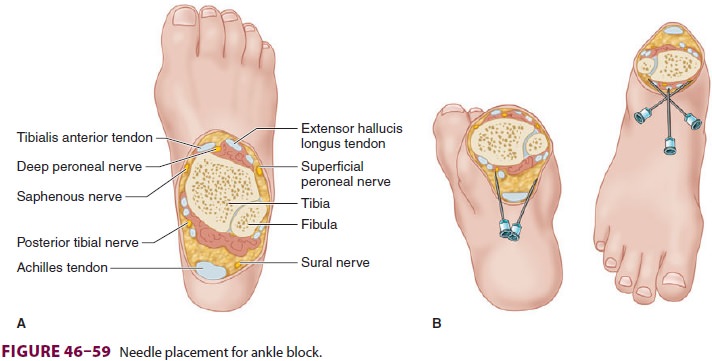
A complete ankle block requires a series of
five nerve blocks, but the process may be streamlined
to minimize needle insertions (Figure 46–59).
All five injections are required to anesthetize the entire foot; however, many
surgical procedures involve only a few terminal nerves, and only affected
nerves should be blocked. In addition, unlike a sci-atic nerve block, an ankle
block provides no analge-sia for (below-the-knee) tourniquet pain, nor does it
allow for perineural catheter insertion. To block the deep peroneal nerve, the
groove between the exten-sor hallucis longus and extensor digitorum longus
tendons is identified. The dorsalis pedis pulse is often palpable here. A
short, small-gauge block nee-dle is inserted perpendicular to the skin just
lateral to the pulse, bone is contacted, and 5 mL of local anesthetic is
infiltrated as the needle is withdrawn. Continuing from this insertion site, a
subcutaneous wheal of 5 mL of local anesthetic is extended toward the lateral
malleolus to target the superficial pero-neal nerve. The needle is withdrawn
and redirected from the same location in a medial direction, infil-trating 5 mL
of local anesthetic toward the medial malleolus to target the saphenous nerve.
The poste-rior tibial nerve may be located by identifying the posterior tibial
artery pulse behind the medial mal-leolus. A short, small-gauge block needle is
inserted just posterior to the artery and 5 mL of local anes-thetic is
distributed in the pocket deep to the flexor retinaculum. To target the sural
nerve, 5 mL of local anesthetic is injected subcutaneously posterior to the
lateral malleolus.
Related Topics