Chapter: Psychology: Development
Cognitive Changes in Adulthood
Cognitive Changes in Adulthood
Life
expectancies have increased dramatically. In the years of the Roman Empire,
people lived only two or three decades; early in the twentieth century, death
by age 40 was common. By 1955, worldwide life expectancy had reached 48 years;
the world aver-age was 68 in 1998 and is far beyond that today in many
countries (WHO, 1998). These demographic changes mean that a larger proportion
of the world’s population is old than ever before, and this has encouraged a
growing interest in the nature of age-related changes in cognitive functioning,
as well as the steps that can be taken to halt or even reverse the decline
associated with aging. A number of encouraging early studies have suggested
predictors of “successful aging” and other studies have offered mental training
programs or strategies that can help people retain and improve their cognitive
abilities (Baltes, Staudinger, & Lindenberger, 1999; Freund & Baltes,
1998; Hertzog, Kramer, Wilson, & Lindenberger, 2009). To appreciate this
work, we need to consider how cognitive performance changes with age.
CHANGES IN INTELLECTUAL PE RFORMANCE
Failing
memory has long been considered an unavoidable part of aging. However, some
aspects of memory—including implicit memory and some measures of semantic
memory—show little or no decline with aging. Age-related declines are evident,
however, in measures of working memory and episodic memory (see, for example,
Earles, Connor, Smith, & Park, 1998). The elderly also have trouble in accessing their memories; in fact, one
of the most common complaints associated with aging is the difficulty in
recalling names or specific words (G. Cohen & Burke, 1993).
The
broader decline in intellectual functioning is similarly uneven—the key
difference is between fluid and crystallized intelligence. As noted, fluidintelligence refers to a person’s
ability to deal with new and unusual problems, whereas crystallized intelligence refers to a person’s accumulated
knowledge, including his vocab-ulary, the facts he knows, and the strategies he
has learned.
Crystallized
intelligence remains relatively stable across the life span and, in some
stud-ies, seems to grow as the individual gains life experience. Fluid
intelligence shows a very dif-ferent pattern. The decline starts when the
person is in his twenties and continues as the years go by (Figure 14.39).
However, the decline is gradual, and many individuals maintain much of their
intellectual capacity into their sixties and seventies (Craik & Salthouse,
2000; Salthouse, 2000, 2004; Schaie, 1996; Verhaeghen & Salthouse, 1997).
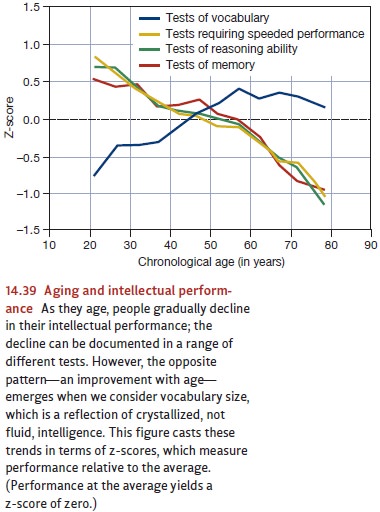
Figure
14.39 suggests that the decline in mental capacities proceeds steadily across
much of the life span. Why, therefore, do we notice the decline primarily in
the elderly? Why do people often lament the loss of cognitive capacities
between ages 60 and 80, but not comment on the similar drop-off between ages 20
and 40? One reason is that as one
matures, gains in crystallized
intelligence often compensate
for declines in fluid intelligence. Thus, as the years pass, people
master more and more strategies that help them in their daily functioning, and
this balances out the fact that their thinking is not as nimble as it used to
be. In addition, 30- or 40-year-olds might be less able than 20-year-olds, but
we do not detect the decline because the 30- or 40- year-olds still have more
than adequate capacity to manage their daily routines. We
detect cognitive decline
only later, when
the gradual drop-off in
mental skills eventually
leaves people with
insufficient capacity to handle their daily chores (Salthouse, 2004).
Common sense also
suggests that people
differ markedly in
how they age—some show a dramatic drop in mental
capacities but others experience very little loss. This may be an instance in
which common sense doesn’t match the facts. If we focus on individu- als who
are still reasonably
active and who
describe themselves as
being in “good
to
excellent
health,” then we find impressive consistency from one individual to the next in
how they are affected by the passing years (Salthouse, 2004). Put differently,
the drop- off we see in Figure 14.39 is not the result of a few unfortunate
individuals who rapidly lose their abilities and pull down the average.
Instead, the decline seems to affect most people, to roughly the same degree.
CAUSES OF AGE - RELATED DECLINES INCOGNITIVE FUNCTIONING
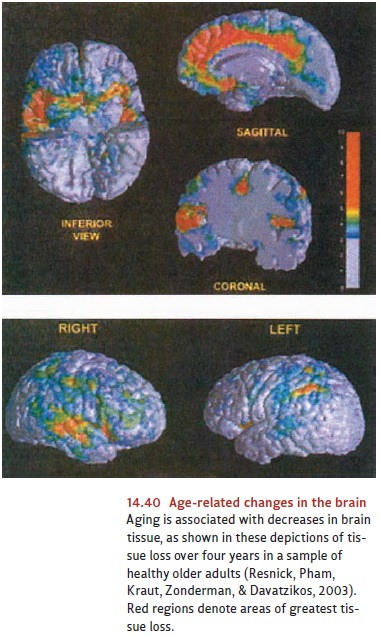
What
factors are responsible for age-related cognitive declines? Some investigators
pro- pose biological explanations, cast in terms of age-related changes in
blood flow or neu- roanatomy, or the gradual death of neurons across the life
span (Figure 14.40; Resnick et al., 2003).
Still others have
suggested that the
cause of many
of these cognitive changes is an age-related decline
in working memory or the capacity for paying atten- tion (Craik &
Bialystok, 2006). In fact, all of these hypotheses may be correct, and each may
describe one of the factors that governs how individuals age.
The
way each individual ages is also shaped by other factors. One factor is the
degree of stimulation in the individual’s life (Schaie & Willis, 1996);
those who are less stim- ulated are more vulnerable to the effects of aging. Also relevant are a wide variety of
medical factors. This reflects the fact that the cells making up the central
nervous sys- tem can function only if they receive an ample supply of oxygen
and glucose. (In fact, the brain consumes
almost 20% of
the body’s metabolic
energy, even though
it accounts for only about 2 or 3% of the overall body weight.) As a
result, a wide range of bodily changes that diminish the availability of these
resources can also impair brain functioning. For example, a decline in kidney
function will have an impact throughout the body, but because of the brain’s
metabolic needs, the kidney problem may lead to a loss in
mental functioning well
before other symptoms
appear. Likewise, circulatory problems (including problems with the
heart itself or hardening of the arteries) will obviously diminish the
quantity and quality of the brain’s blood supply, and so can con- tribute to a
cognitive decline (see, for example, Albert et al., 1995).
Finally, cognitive
functioning in the
elderly is also
affected by a
number of age- related diseases, including Alzheimer’s disease, a disorder
characterized by a progres- sive and widespread loss of nerve cells, leading to
memory problems, disorientation, and, eventually, total helplessness. Evidence
has made it clear that genetic factors can increase someone’s risk of
Alzheimer’s disease (Goedert & Spillantini, 2006), but its exact causes
remain uncertain.
These
declines may sound downright discouraging, because they highlight the many
fronts on which we are all vulnerable to aging, but there are ways to slow the
process. For example, physical exercise has been shown to be good for not only
the body (maintaining muscle strength and tone, as well as cardiovascular
fitness) but also the mind. Although fitness programs are not a cure-all for
the effects of aging, physical exercise can, in many cases, help preserve
mental functioning in the elderly (Colcombe & Kramer, 2003; Cotman &
Neeper, 1996; A. F. Kramer & Willis, 2002). There is also a growing
literature on the effi-cacy of mental
exercise, although the jury is still out on the extent and breadth of gains
associated with mental exercise (Salthouse, 2006, 2007; Schooler, 2007).
Related Topics