Chapter: Introduction to Human Nutrition: Minerals and Trace Elements
Sodium and chloride: Absorption, transport, tissue distribution, Metabolic function, essentiality, Deficiency symptoms
Sodium and chloride
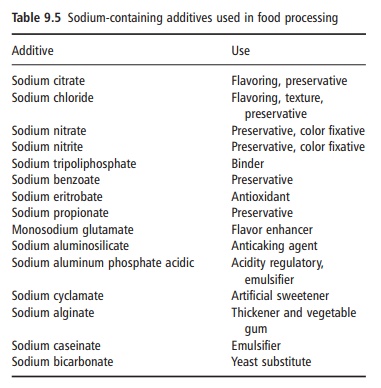
Sodium is the sixth most abundant element in the Earth’s crust and salt (sodium chloride) makes up about 80% of the dissolved matter in seawater. Although there is a wide variety of sodium salts, many of which are used as additives in food processing (e.g., sodium nitrate and monosodium glutamate), sodium chloride is the major source of sodium in foods. As sodium and chloride intakes in humans are so closely matched, both will be considered together in this text.
Salt was of major importance in early civilizations and in prehistory. Humans have special taste and salt appetite systems, which led to special culinary uses for salt and made it a much sought-after commodity. Nowadays, salt is still used widely to modify flavor, to alter the texture and consistency of food, and to control microbial growth (Table 9.5).
Absorption, transport and tissue distribution
Sodium is the major extracellular electrolyte and exists as the fully water-soluble cation. Chloride is also mainly found in ECF and is fully water soluble as the chloride anion. Both ions are readily absorbed from the digestive tract. Glucose and anions such as citrate, propionates, and bicarbonate enhance the uptake of sodium. The “average” 70 kg male has about 90 g of sodium with up to 75% contained in the mineral apatite of bone. Plasma sodium is tightly regulated through a hormone system, which also regulates water balance, pH, and osmotic pressure.
Angiotensin and aldosterone both act to conserve sodium by increasing sodium reabsorption by the kidney. Sodium depletion stimulates the renal pro-duction of renin, which generates active angiotensin in the circulation. The latter stimulates vasoconstric-tion, which increases blood pressure, decreases water loss, and stimulates aldosterone release from the adrenal cortex. Atrial natriuretic hormone counter-acts the sodium retention mechanisms by suppressing renin and aldosterone release and by inducing water and sodium excretion. It also decreases blood pres-sure and antagonizes angiotensin. A raised plasma sodium concentration stimulates the renal reabsorp-tion of water and decreases urinary output via antidiuretic hormone from the posterior pituitary. In contrast to sodium, chloride is passively distributed throughout the body and moves to replace anions lost to cells via other processes.
The main excretory route for both sodium and chloride is the urine. Sweat loss of these ions tends to be very low except with severe exertion in hot climates. Fecal losses are also low in healthy individuals.
Metabolic function and essentiality
The sodium cation is an active participant in the reg-ulation of osmotic and electrolyte balances, whereas the chloride anion is a passive participant in this regu-latory system. Each ion, however, has other functions within the body.
Sodium is involved in nerve conduction, active cel-lular transport and the formation of mineral apatite of bone. Central to its role in water balance, nerve conduction, and active transport is the plasma mem-brane enzyme sodium–potassium-ATPase (Na+/K+-ATPase). This enzyme pumps sodium out of the cell and at the same time returns potassium to the intra-cellular environment while ATP is hydrolyzed. Signal transmission along nerve cells, active transport of nutrients into the enterocyte and muscle contraction/ relaxation all depend on the Na+/K+-ATPase pump. In the muscle there is an additional pump, the sodium– calcium system. The ATP utilized by the sodium pump makes up a substantial part of the total meta-bolic activity and thermogenesis.
Among the main functions of the chloride anion are as dissociated hydrochloric acid in the stomach and in the chloride shift in the erythrocyte plasma membrane, where it exchanges with the bicarbonate ion.
Deficiency symptoms
Obligatory losses of sodium are very low, and low plasma sodium or chloride depletion is difficult to induce. Low plasma sodium or chloride is not diet related but rather caused by a variety of clinical conditions, including major trauma and cachexia and overuse of diuretics. Loss of sodium can also ensue as a result of excessive water intake, anorexia nervosa, ulcerative colitis, liver disease, congestive heart failure with edema, and severe infection and diarrhea. Acute diarrhea is the most common cause of sodium deficiency, and oral rehydration depends on the efficient enteric uptake of sodium from iso-tonic glucose/saline solutions and saves many lives worldwide. Vomiting, chronic renal disease, renal failure, and chronic respiratory acidosis can result in chloride depletion.
Related Topics