Chapter: Clinical Anesthesiology: Regional Anesthesia & Pain Management: Peripheral Nerve Blocks
Lower Extremity Peripheral Nerve Blocks: Posterior Lumbar Plexus (Psoas Compartment) Block
Posterior Lumbar Plexus (Psoas Compartment) Block
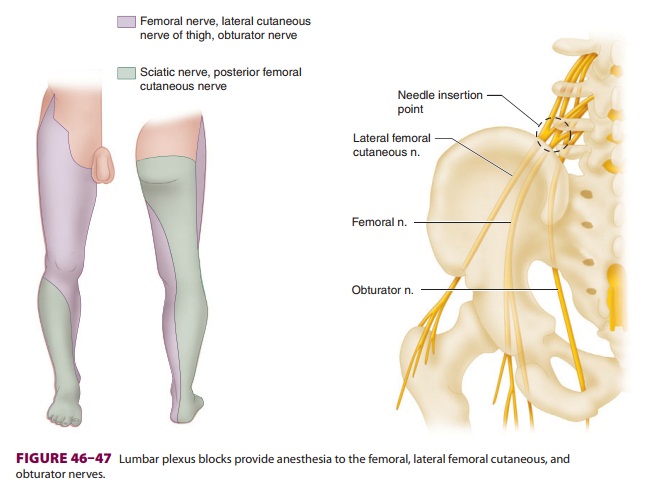
Posterior lumbar plexus blocks are useful for
surgical procedures involving areas innervated by the femoral, lateral femoral
cutaneous, and obturator nerves ( Figure 46–47).
These include
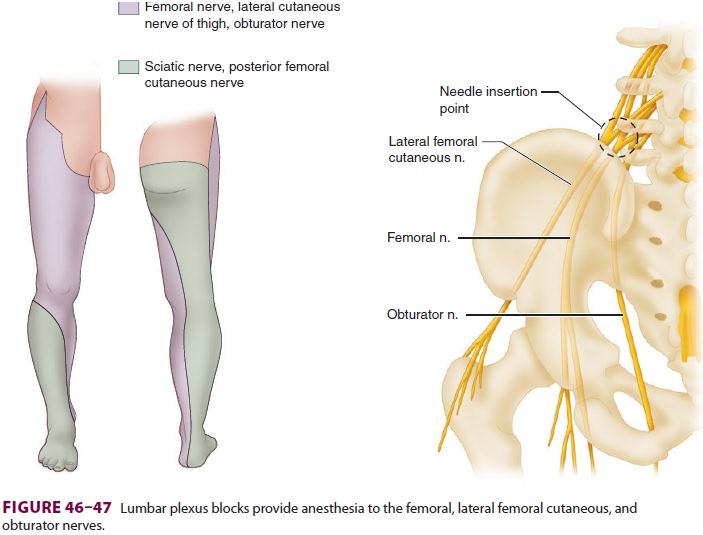
procedures on the hip, knee, and anterior thigh. Complete anesthesia of
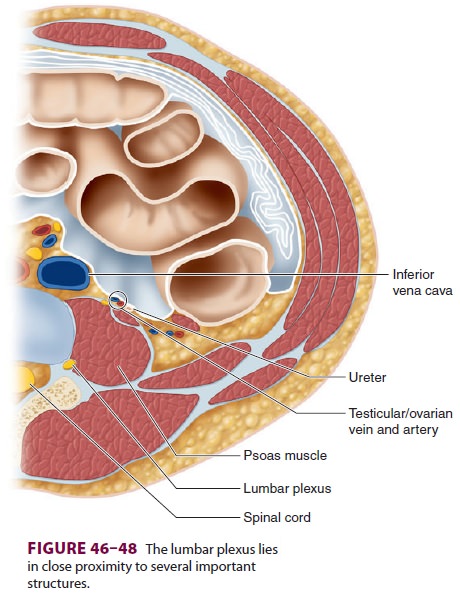
the knee can be attained with a proximal sciatic nerve block. The lumbar plexus
is relatively close to multiple sensitive struc-tures (Figure
46–48) and reaching it requires a very long needle.
Hence, the posterior lumbar plexus block has one of the highest complication
rates of any peripheral nerve block; these include retroperi-toneal hematoma,
intravascular local anesthetic injection with toxicity, intrathecal and
epidural injections, and renal capsular puncture with subse-quent hematoma.
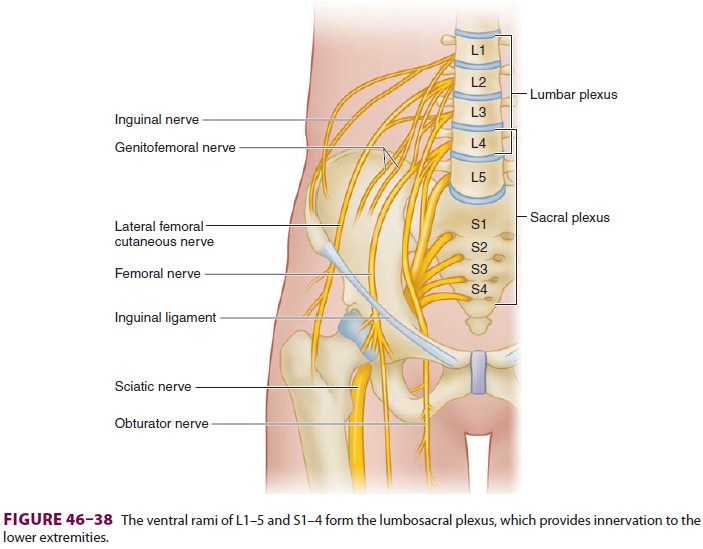
Lumbar nerve roots emerge into the body of
the psoas muscle and travel within the muscle com-partment before exiting as
terminal nerves (see Figure 46–38). Modern posterior lumbar plexus blocks
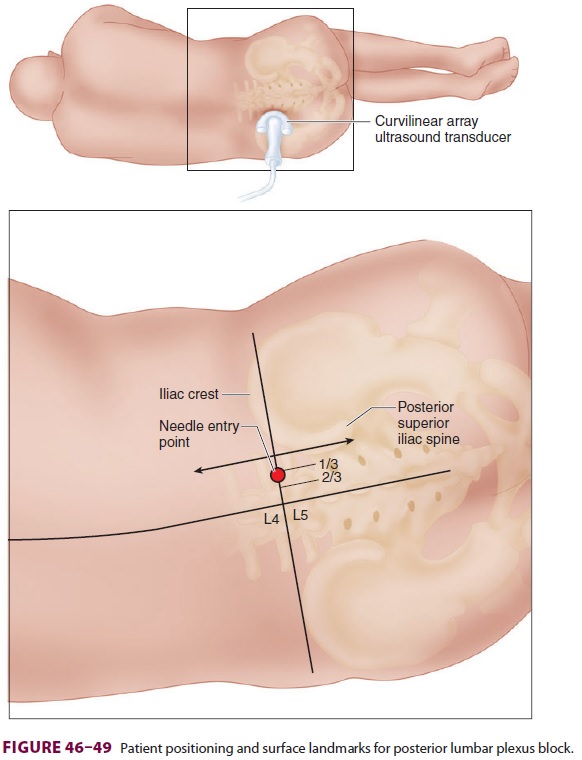
deposit local anesthetic within the body of the psoas muscle. The patient is
positioned in lateral decubitus with the side to be blocked in the
non-dependent position (Figure 46–49). The midline is palpated, identifying the
spinous processes if possi-ble. A line is first drawn through the lumbar
spinous processes, and both iliac crests are identified and connected with a
line to approximate the level of L4. The posterior superior iliac spine is then
palpated and a line is drawn cephalad, parallel to the first line. If
available, ultrasound imaging of the transverse process may be helpful to
estimate lumbar plexus depth. A long (10- to 15-cm) insulated needle is
inserted at the point of intersection between the transverse (intercristal)
line and the intersection of the lateral and middle thirds of the two sagittal
lines. The needle is advanced in an anterior direction until a femoral motor
response is elicited (quadri-ceps contraction). If the transverse process is
con-tacted, the needle should be withdrawn slightly
and “walked off ” the transverse process in a
caudal direction, maintaining the needle in the parasagit-tal plane. The needle
should never be inserted more than 3 cm past the depth at which the transverse
process was contacted. Local anesthetic volumes greater than 20 mL will
increase the risk of bilateral spread and contralateral limb involvement.
Related Topics