Chapter: Biology of Disease: Disorders of the Immune System
Systemic Lupus Erythematosus - Autoimmune Disorders
SYSTEMIC LUPUS ERYTHEMATOSUS
Systemic lupus erythematosus (SLE) is an autoimmune
disease in which about 95% of patients have antinuclear antibodies (ANAs) in
their plasma. The deposition of immune complexes leads to widespread
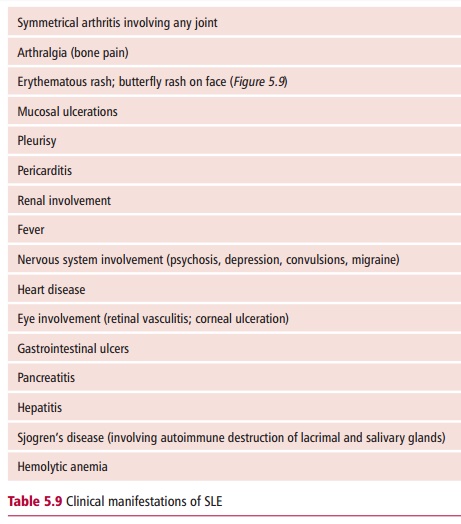
inflammation that affects many organs systems within the body. Clinical
features of the disease are summarized in Table
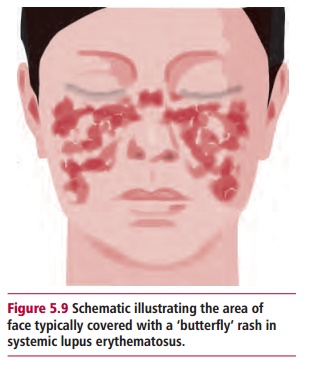
5.9, the commonest presentations are arthritis and skin rash, particularly
the butterfly rash of the face (Figure
5.9). Renal disease occurs in
approximately half of affected individuals, with nephritis developing early on
in the disease. Although the etiology of SLE is uncertain, the systemic nature
of the disease is linked to the type of autoantibodies present. The disease
primarily affects women of reproductive age, although much younger and much
older patients have been seen. The female to male ratio is about 4 : 1, although
in younger patients this gender bias does not occur.
Unfortunately different patients have different patterns of symptoms and their variety in this multisystem disorder has, in the past, presented difficulties with diagnosis, so it must take full
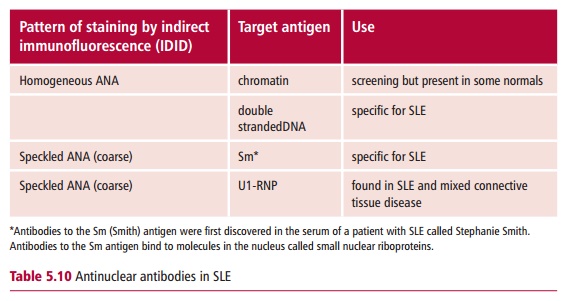
account of the range of presentations. Diagnosis can be helped by demonstrating
the presence of ANAs in samples of plasma, using indirect immunofluorescence on
cultured Hep-2 cells. The commonest pattern seen is a diffuse staining
throughout the nucleus due to antibodies against chromatin. It is also possible
to detect different patterns of fluorescence which are indicative of antibodies
to different nuclear antigens and which can help in diagnosis or in assessing
prognosis (Table 5.10).
Autoantibodies against extractable
nuclear antigens(ENA) can also be detected by RIA or ELISA . Positive tests
forANAs require further investigations, for example with tests for
antidouble-stranded dsDNA (dsDNA) antibodies. The presence in the blood of
so-called LE cells, which are neutrophils containing phagocytozed nuclei and
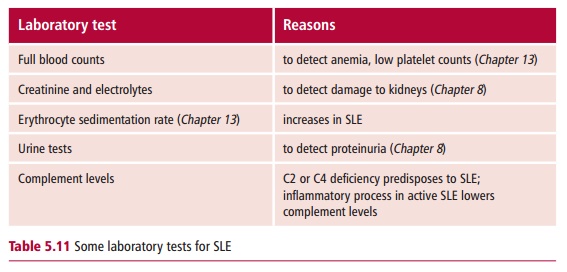
resemble large multinucleate cells, is also indicative of SLE. Other laboratory
tests used in the diagnosis of SLE include those listed in Table 5.11. Rheumatoid
factor and the presence of antibodies against
cardiolipin may also be present, although these are not specific for SLE.
Systemic lupus erythematosus is treated with
immunosuppressive drugs, such as azathioprine or cyclosporine although the use
of such drugs in patients prone to kidney disease needs careful monitoring. In
addition, patients maintained on immunotherapy are more susceptible to
infectious diseases. The prognosis for sufferers of SLE has improved greatly
over the last 50 years because the disease is now diagnosed earlier. For
example, in the 1950s, most patients died within 10 years of diagnosis, whereas
today around 90% are alive 10 years after diagnosis.
Related Topics