Chapter: Orthopaedics
Orthopaedics: Elbow
Elbow
General Principles
·
articulation between distal humerus, proximal
ulna. proDmal radiUll (humeromdial, humeroulnar and radioulnar joints)
·
fractures and dislocations of the elbow are
evident on AP, lateral and oblique radiographs
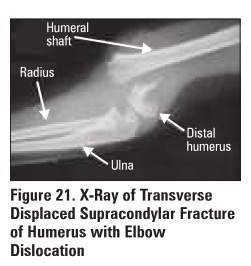
Supracondylar Fracture
·
most common in pediatric population (peak age -7
years old), rarely seen in adults
·
anterior interosseous nerve (AIN) injury commonly associated
with extension type
Mechanism
·
>96% are extension injuries via FOOSH (e.g.
fall off monkey bars); <496 are flexion Injuries
Clinical Features
·
pain. swelling. point tenderness
·
neurovascular Injury- assess median and radial
nerve, radial artery
Investigations
·
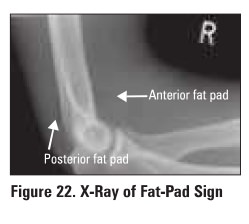
x-rays: AP, lateral of elbow; assess for fat pad
sign
Treatment
·
non-operative
o
nondisplaced: cast in 900 :flexion for 3 weeks
·
operative
o
Indications: displaced, vascular injury, open fracture
o
requires perc11taneous pinning followed by limb
cast with elbow flexed >90"
o
in adults, ORIF is necessary
Specific Complications (see
General Fracture Complications)
·
brachial artery injury, median or ulnar nerve
injury, compartment syndrome (leads to Volkmann's ischemic contracture),
malallgnment cubitus varus (distal fragment tilted into varus)
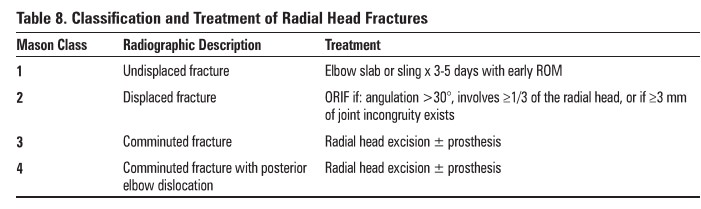
Radial Head Fracture
·
a common fracture of the upper limb in young
adults
Mechanism
·
FOOSH with elbow extended and forearm pronated
Clinical Features
·
marked local tenderness on palpation over radial
head (lateral elbow)
·
decreased ROM at elbow, mechanical block to forearm
pronation and supination
·
pain on pronation/supination
Investigations
·
x-ray: enlarged anterior fat pad ("sail"
sign") or the presence ofa posterior fat pad indicate occult radial head
fractures
Specific Complications (see
General Fracture Complications)
·
myositis ossificans
·
recurrent inst8bility (if medial collateral
ligament injured and radial head excised)
Olecranon Fracture
Mechanism
·
direct trauma to posterior aspect of elbow (fall
onto the point of the elbow)
Clinical Features
·
± loss of active extension due to avulsion of
triceps tendon
Treatment
·
undisplaced ( <2 mm, stable): cast x 3 weeks
(elbow in 45° flexion) then gentle ROM
·
displaced: ORIF (plate and Screws or tension band
wiring) and early ROM if stable
Elbow Dislocation
·
third most common joint dislocation after shoulder
and patella
·
most commonly occurs in young people (5-25 yean)
in sporting events or high speed MVAs, dislocation of ulna
·
90% are posterior/posterolateral, anterior are
rare
·
collateral ligaments disrupted
Mechanism
·
elbow hyperextension via FOOSH or
valgus/supination stress during elbow flexion
Clinical Features
·
elbow pain, swelling. Deformity
·
flexion contracture
·
± absent radial or ulnar pulses
Treatment
·
closed reduction under anesthesia (pori-reduction
x-rays required)
·
long-arm splint with forearm in neutral rotation
and elbow in 90 degree flexion
·
early ROM (<2 weeks)
Specific Complications (see
General Fracture Complications)
·
sti1fness (loss of extension), intra-articular
loose body, neurovascular injury (ulnar nerve, median nerve, brachial artery),
radial head fracture
Epicondylitis
·
lateral epicondylitis = "tennis elbow",
inflammation of the common extensor tendon as it inserts into the lateral
epicondyle
·
medial epicondylitis = "golfer's elbow':
inflammation of the common flexor tendon as it inserts into the medial
epicondyle
Mechanism
·
repeated or sustained contraction of the forearm muscles
Clinical Features
·
point tenderness over humeral epicondyle
·
pain upon resisted wrist extension (lateral
epicondylitis) or wrist flexion (medial epicondylitis)
·
generally a self-limited condition. but may take
6-18 months to resolve
Treatment
·
rest, ice, NSAIDs
·
use brace/strap
·
PT, stretching and strengthening
·
corticosteroid injection
·
Surgery: percutaneous or open release of common
tendon from epicondyle (only after 6-12 months of conservative therapy)
Related Topics