Chapter: Basic & Clinical Pharmacology : Cancer Chemotherapy
Deoxycytidine Analogs
DEOXYCYTIDINE ANALOGS
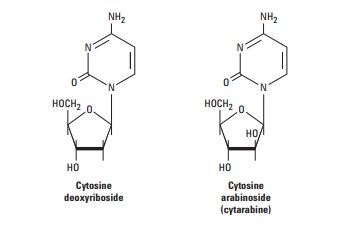
Cytarabine
Cytarabine (ara-C) is an S phase-specific antimetabolite that is con-verted by deoxycytidine kinase to the 5'-mononucleotide (ara-CMP). Ara-CMP is further metabolized to the diphosphate and triphos-phate metabolites, and the ara-CTP triphosphate is felt to be the main cytotoxic metabolite. Ara-CTP competitively inhibits DNA polymerase-α and DNA polymerase-β, thereby resulting in blockade of DNA synthesis and DNA repair, respectively. This metabolite is also incorporated into RNA and DNA. Incorporation into DNA leads to interference with chain elongation and defective ligation of fragments of newly synthesized DNA. The cellular retention of ara-CTP appears to correlate with its lethality to malignant cells.
After intravenous
administration, the drug is cleared rapidly, with most of an administered dose
being deaminated to inactive forms. The stoichiometric balance between the
level of activation and catabolism of cytarabine is important in determining
its even-tual cytotoxicity.
The clinical activity
of cytarabine is highly schedule-dependent and because of its rapid
degradation, it is usually administered via continuous infusion over a 5–7 day
period. Its activity is limited exclusively to hematologic malignancies,
including acute myelog-enous leukemia and non-Hodgkin’s lymphoma. This agent
has absolutely no activity in solid tumors. The main adverse effects associated
with cytarabine therapy include myelosuppression, mucositis, nausea and
vomiting, and neurotoxicity when high-dose therapy is administered.
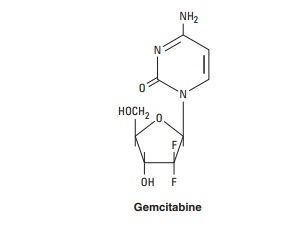
Gemcitabine
Gemcitabine is a fluorine-substituted deoxycytidine analog that is phosphorylated initially by the enzyme deoxycytidine kinase to the monophosphate form and then by other nucleoside kinases to the diphosphate and triphosphate nucleotide forms. The antitu-mor effect is considered to result from several mechanisms: inhibi-tion of ribonucleotide reductase by gemcitabine diphosphate, which reduces the level of deoxyribonucleoside triphosphates required for DNA synthesis; inhibition by gemcitabine triphos-phate of DNA polymerase-α and DNA polymerase-β, thereby resulting in blockade of DNA synthesis and DNA repair; and incorporation of gemcitabine triphosphate into DNA, leading to inhibition of DNA synthesis and function. Following incorpora-tion of the gemcitabine triphosphate into DNA, only one addi-tional nucleotide can be added to the growing DNA strand, resulting in chain termination.
This nucleoside analog was initially approved for use in advanced pancreatic cancer but is now widely used to treat a broad range of malignancies, including non-small cell lung cancer, blad-der cancer, ovarian cancer, soft tissue sarcoma, and non-Hodgkin’s lymphoma. Myelosuppression in the form of neutropenia is the principal dose-limiting toxicity. Nausea and vomiting occur in 70% of patients and a flu-like syndrome has also been observed. In rare cases, renal microangiopathy syndromes, including hemo-lytic-uremic syndrome and thrombotic thrombocytopenic pur-pura have been reported.
Related Topics