Chapter: Clinical Dermatology: Regional dermatology
The nails Infections
Infections
Acute paronychia
The
portal of entry for the organisms concerned, usually staphylococci, is a break
in the skin or cuticle as a result of minor trauma. The subsequ-ent acute
inflammation, often with the formation of pus in the nail fold or under the
nail, requires systemic treatment with flucloxacillin or erythro-mycin and appropriate surgical drainage.
Chronic paronychia
Cause
A
combination of circumstances can allow a mixture of opportunistic pathogens
(yeasts, Gram-positive cocci and Gram-negative rods) to colonize the space
between the nail fold and nail plate. Predisposing fac-tors include a poor
peripheral circulation, wet work, working with flour, diabetes, vaginal
candidosis and overvigorous cutting back of the cuticles.
Presentation and course
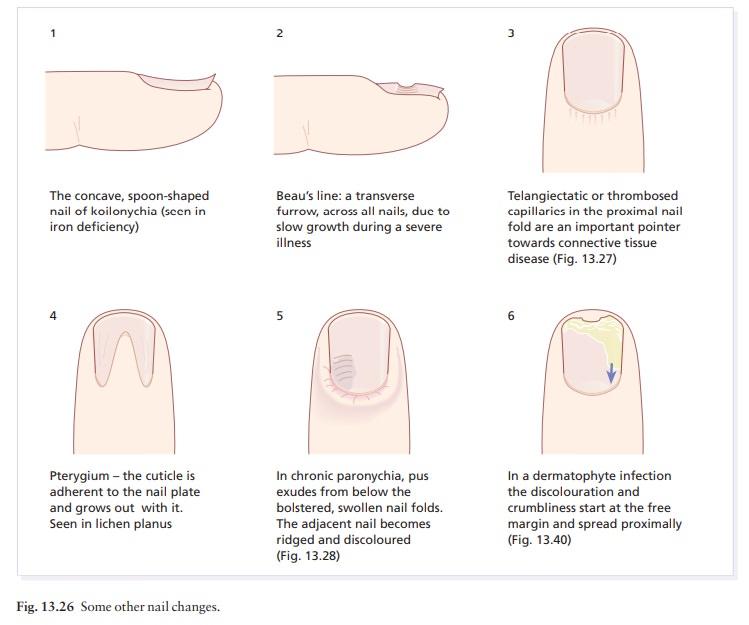
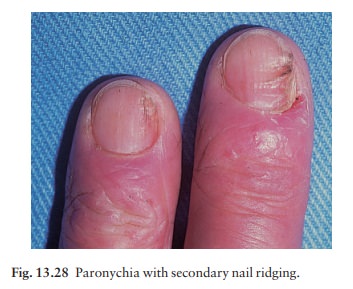
The
nail folds become tender and swollen (Figs 13.26 and 13.28) and small amounts
of pus are discharged at intervals. The cuticular seal is damaged and the
adjacent nail plate becomes ridged and discoloured. The condition may last for
years.
Differential diagnosis
In atypical cases, consider the outside chance of an amelanotic melanoma. Paronychia should not be con-fused with a dermatophyte infection in which the nail folds are not primarily affected.
Investigations
Test the urine for sugar, check for vaginal candidosis.
Pus
should be cultured.
Treatment
Manicuring
of the cuticle should cease. The hands should be kept as warm and as dry as
possible, and the damaged nail folds packed several times a day with an
imidazole cream. If there is no response, and swabs confirm that candida is
present, a 2-week course of itraconazole should be considered.
Dermatophyte infections (Figs
13.26 and 14.40)
Cause
The
common dermatophytes that cause tinea pedis can also invade the nails.
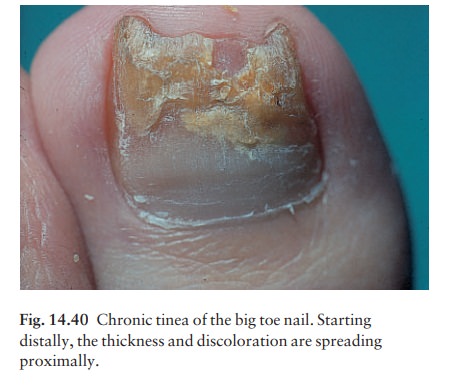
Presentation
Toenail
infection is common and associated with tinea pedis. The early changes occur at
the free edge of the nail and spread proximally. The nail plate becomes yellow,
crumbly and thickened. Usually only a few nails are infected but occasionally
all are. The fingernails are involved less often and the changes, in contrast
to those of psoriasis, are usually confined to one hand.
Clinical course
The
condition seldom clears spontaneously.
Differential diagnosis
Psoriasis
has been mentioned. Yeast infections of the nail plate, much more rare than
dermatophyte infec-tions, can look similar. Coexisting tinea pedis favours
dermatophyte infection of the nail.
Investigations
Microscopic
examination of a nail clipping is a simple procedure. Cultures should be
carried out in a mycology laboratory.
Treatment
Remember
that most symptom-free fungal infections of the toenails need no treatment at
all.
Tumours
Peri-ungual warts are common and stubborn. Cryo-therapy must be used carefully to avoid damage to the nail matrix. It is painful but effective.
Peri-ungual
fibromas (see Fig. 21.5) arise from thenail folds, usually in late
childhood, in patients with tuberous sclerosis.
Glomus
tumours can occur beneath the nail plate.The small red or bluish
lesions are exquisitely painful if touched and when the temperature changes.
Treat-ment is surgical.
Subungual
exostoses (Fig. 13.22) protrude painfullyunder the nail plate. Usually
secondary to trauma to the terminal phalanx, the bony abnormality can be seen
on X-ray and treatment is surgical.
Myxoid
cysts (Fig. 13.29) occur on the proximalnail folds, usually of the
fingers. The smooth domed swelling contains a clear jelly-like material that
tran-silluminates well. A groove may form on the adjacent nail plate.
Cryotherapy, injections of triamcinolone and surgical excision all have their
advocates.

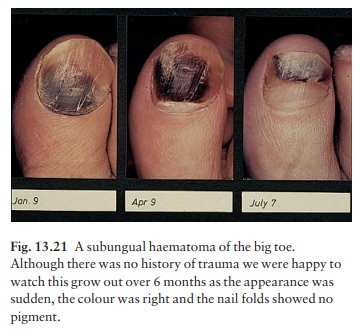
Malignant melanoma should be suspected in any subungual pigmented lesion, particularly if the pigment spreads to the surrounding skin. Subungual haematomas may cause confusion but ‘grow out’ with the nail (Fig. 13.21). The risk of misdiagnosis is high-est with an amelanotic melanoma, which may mimic chronic paronychia or a pyogenic granuloma.
Related Topics