Chapter: Clinical Dermatology: Regional dermatology
Alopecia areata
Alopecia areata
This
affects about 2% of the patients seen at our skin clinics.
Cause
An immunological basis is suspected because of an association with thyroid disease, vitiligo and atopy.
Histologically,
T lymphocytes cluster like a swarm of bees around affected hair bulbs, having
been attracted and made to divide by cytokines from the dermal papilla.
Alopecia areata is probably inherited as a complex genetic trait, with an
increased occurrence in the first-degree relatives of affected subjects and
twin concordance. The existence of trigger factors, such as stress, fits with
this idea.
Presentation
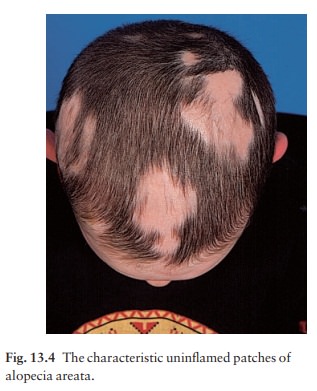
A
typical patch is uninflamed, with no scaling, but with easily seen empty hair
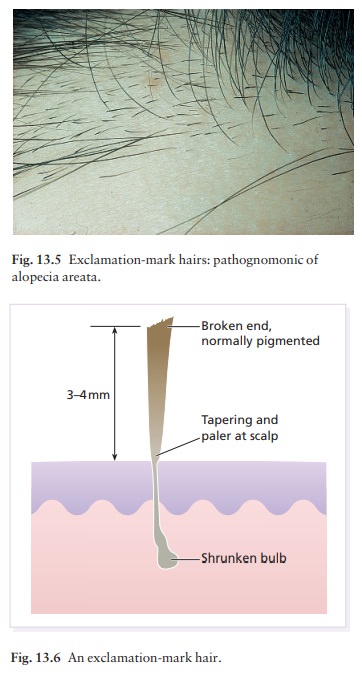
follicles (Fig. 13.4). Pathog-nomonic ‘exclamation-mark’ hairs may be seen
around the edge of enlarging areas. They are broken off about 4 mm from the
scalp, and are narrowed and less pigmented proximally (Figs 13.5 and 13.6).
Patches are most common in the scalp and beard but other areas, especially the
eyelashes and eyebrows, can be affected too. An uncommon diffuse pattern is
recognized, with exclamation-mark hairs scattered widely over a dif-fusely
thinned scalp. Up to 50% of patients show fine pitting or wrinkling of the
nails.
Course
The outcome is unpredictable. In a first attack, regrowth is usual within a few months.
New hairs appear
in the centre of patches as fine pale down, and gradually regain their normal
thickness and colour, although the new hair may remain white in older
pati-ents. Subsequent episodes tend to be more extensive and regrowth is
slower. Hair loss in some areas may coexist with regrowth in others. A few
patients lose all the hair from their heads (alopecia totalis) or from the
whole skin surface (alopecia universalis).
Regrowth
is tiresomely erratic but the following suggest a poor prognosis.
1 Onset
before puberty.
2 Association
with atopy or Down’s syndrome.
3
Unusually widespread alopecia.
4 Involvement
of the scalp margin (ophiasiform type), especially at the nape of the neck.
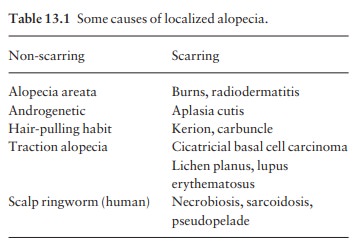
Differential diagnosis
Patches
are not scaly, in contrast to ringworm, and are usually uninflamed, in contrast
to lupus erythematosus and lichen planus. In the hair-pulling habit of
children, and in traction alopecia, broken hairs may be seen but true
exclamation-mark hairs are absent. Secondary syphilis can also cause a
‘moth-eaten’ patchy hair loss.
Investigations
None
are usually needed. Syphilis can be excluded with serological tests if
necessary. Organ-specific auto-antibody screens provide interesting information
but do not affect management.
Treatment
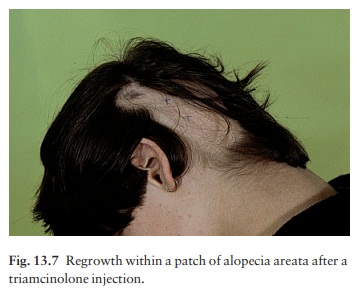
A patient with a first or minor attack can be reassured about the prospects for regrowth. Tranquillizers may be helpful at the start. The use of systemic steroids should be avoided in most cases, but the intradermal injection of 0.2 mL of intralesional triamcinolone acetonide (10 mg /mL), raising a small bleb within an affected patch, leads to localized tufts of regrowth (Fig. 13.7) while not affecting the overall outcome. This may be useful to re-establish eyebrows or to stimulate hope. Spirit-based steroid lotions and mild irritants, such as 0.1–0.25% dithranol, are often used but with limited success.
Ultraviolet radiation or even psoralen with
ultraviolet A (PUVA) therapy may help extens-ive cases, but hair fall often
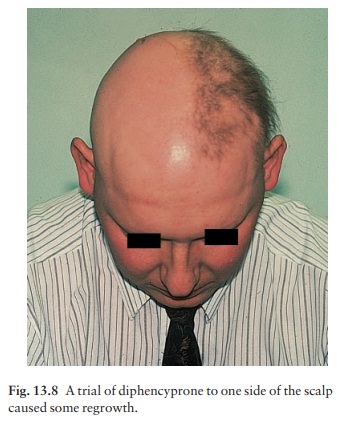
returns when treatment stops. Contact sensitizers (e.g. diphencyprone) seemed
promising (Figs 13.8) but the long-term effect of per-sistent antigen
stimulation is worrying; they are still being used only in a few centres under
trial conditions. The efficacy of topical immunosuppressive agents (e.g.
tacrolimus) has yet to be proved in a randomized clinical trial. Wigs are
necessary for extensive cases.
Related Topics