Chapter: Clinical Dermatology: Regional dermatology
Aphthae
Aphthae
Presentation
These
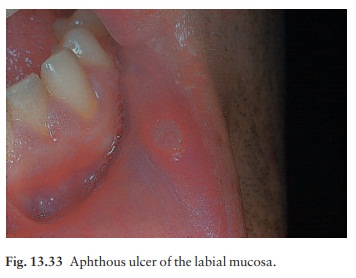
common small oval painful mouth ulcers arise, usually without an obvious cause,
most often in ‘movable mucosae’ such as the gutters of the mouth, tongue or
cheek (Fig. 13.33). An area of tenderness changes into a small red papule that
quickly turns into a grey 2–5 mm painful ulcer with a red areola. Herpetiform
aphthae occur in groups of 2–5 tiny painful ulcers. Major aphthae (periadenitis
mucosa necrotica) are usually larger than 1 cm across and tend to appear in the
back of the mouth.
Course
Small
ulcers heal in a week or two; the pain stops within days. Major aphthae may
persist for months.
Differential diagnosis
Recurrent herpes simplex infections mimic herpetiform apthae but, in the latter, cultures are negative and blisters are not seen. Behçet’s disease causes confusion in patients with major aphthae. In fact, a diagnosis of Behçet’s is often wrongly made in patients with recurrent aphthae of all sorts, when the patient has some other skin disease or joint pain. Patients with true Behçet’s disease should have at least two of these other findings: genital ulcers, pustular vasculitis of skin, synovitis, uveitis or meningoencephalitis.
Investigations
Usually
none are needed. Occasional associations include Crohn’s disease, ulcerative
colitis, gluten-sensitive enteropathy, cyclical neutropenia, other
neutropenias, HIV infection, and deficiencies of iron, vitamin B12
or folate.
Treatment
Prevention
is best. Trauma, such as aggressive tooth brushing, hard or aggravating foods and
stress should be avoided if relevant. The application of a topical
corticosteroid gel, such as fluocinonide, to new lesions may shorten their
course. In severe or complex cases, consider referral.
Related Topics