Chapter: Human Nervous System and Sensory Organs : Diencephalon
Subdivision in Subthalamus
Subthalamus
Subdivision
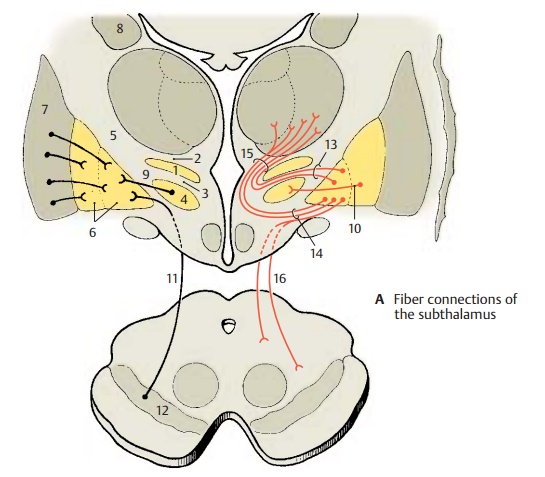
The zona incerta (A1) between Forel’s field H1 (A2) and Forel’s field H2 (A3) is supposed to be a relay station for descending fibers of the globus pallidus.
The subthalamic nucleus (Luys’ body) (A4) between Forel’s field H2 and the internal capsule (A5) has close connec-tions to the pallidum (A6), namely, afferent fibers from the outer segment of the globus pallidus and efferent fibers to the inner seg-ment of the globus pallidus. Bidirectional tracts run to the tegmentum and to the con-tralateral subthalamic nucleus and globus pallidus (supramamillary commissure).
Clinical Note: In humans, injury to the sub-thalamic nucleus leads to hyperkinesis, which may develop into paroxysmal violent flinging movements of the contralateral arm or even the entire body half (hemiballismus, Luys’ body syn-drome). In monkeys, the same symptom complexcan be induced by destroying the subthalamic nucleus.
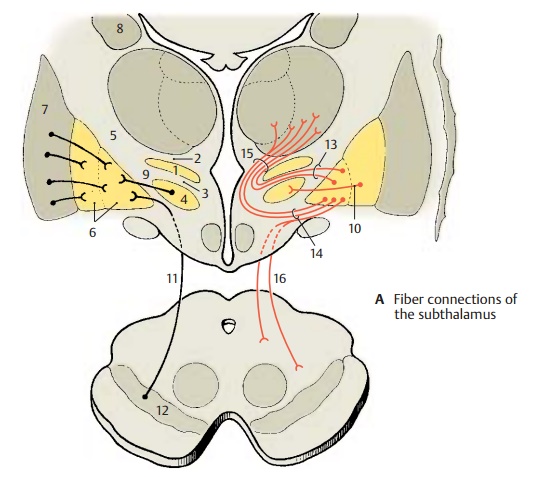
The globus pallidus (Pallidium) (A6) is divided by a myelinated fiber lamella into an outer (lateral) and an inner (medial) segment. Both segments are con-nected by fibers to one another and to the putamen (A7) and the caudate nucleus (A8).Bidirectional connections exist to the sub-thalamic nucleus (A4), with the sub-thalamopallidal fibers (A9) terminating inthe inner segment and the pallidosub-thalamic fibers (A10) originating in the outersegment. Nigropallidal fibers (A11) run from the substantia nigra (A12) to the inner seg-ment of the pallidum.
The lenticular fasciculus (A13) emerges at the dorsal margin of the inner segment of the pallidum and forms Forel’s field H2 ventrally to the zona incerta. The lenticular ansa (A14) emerges from the ventral part of the inner segment and extends in an arch through the inner capsule. Lenticular fasciculus and ansa unite to form the thalamic fasciculus (A15), which formsForel’sfield H1 and radiates into the thalamus (ven-tral anterior nucleus, ventral lateral nucleus, medial nucleus). Fibers from the inner seg-ment of the pallidum run as pallidotegmen-tal tract (A16) into the tegmentum of the midbrain.
Clinical Note: Contrary to the old view thatParkinson’s disease (paralysis agitans) would re-sult from injury to the pallidum, destruction of the pallidum does not lead to motor disorders. Unilateral elimination of the pallidum in patients with Parkinson’s disease removes muscle stiff-ness on the contralateral side and reduces tremor. Bilateral elimination causes mental disorders (postconcussional syndrome: irritability, fatiga-bility, difficulty in concentrating).
Related Topics