Chapter: Clinical Anesthesiology: Perioperative & Critical Care Medicine: Critical Care
Respiratory Failure
Respiratory Failure
Respiratory failure may be defined as
impairment of normal gas exchange severe enough to require acute therapeutic
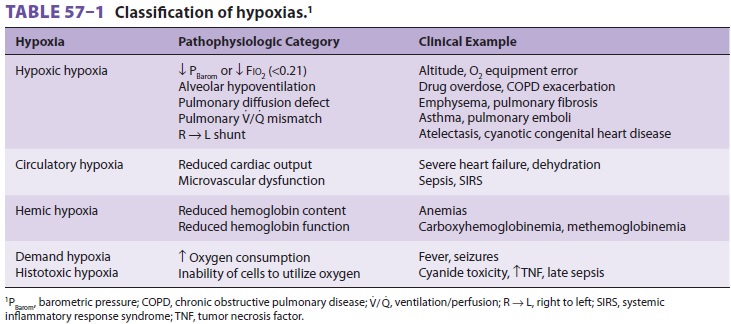
intervention. Definitions based on arterial blood gases (see Table 57–1) may
not apply to patients with chronic pulmonary diseases. For example, dyspnea and
progressive respiratory aci-dosis may be present in patients with chronic CO2 retention. Arterial blood gases typically
follow one of several patterns in patients with respiratory fail-ure (Figure
57–7). At one extreme, the derangement
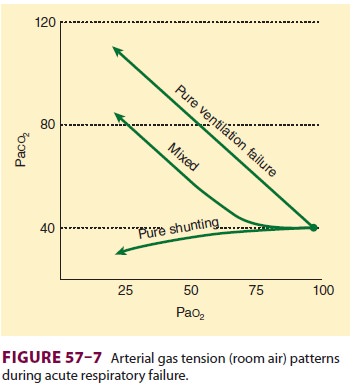
primarily affects oxygen transfer from the
alveoli into blood, giving rise to hypoxemia (hypoxic respi-ratory failure);
unless severe ventilation/perfusion mismatching is present, CO2 elimination in these instances is typically
normal or even enhanced. At the other extreme, the disorder primarily affects
CO2
elimination (pure ventilatory failure), resulting in hypercapnia; mismatching
of ventilation to perfusion is typically absent or minimal. Hypoxemia, however,
can occur with pure ventilatory failure when arte-rial CO2 tension reaches 75–80 mm Hg in patients
breathing room air (see the alveolar gas equation). Few patients with
respiratory failure display a pattern as “pure” as these extreme examples.
Treatment
Regardless of the disorder, the treatment of respi-ratory failure is
primarily supportive while the reversible components of underlying disease are
treated. Hypoxemia is treated with oxygen therapy and positive airway pressure
(if FRC is decreased), whereas hypercarbia (ventilatory failure) is treated
with mechanical ventilation. Other general mea-sures may include using
aerosolized bronchodila-tors, intravenous antibiotics, and diuretics for fluid
overload, therapy to improve cardiac function, and nutritional support.
Related Topics