Chapter: Clinical Anesthesiology: Perioperative & Critical Care Medicine: Critical Care
Prerenal Azotemia
PRERENAL AZOTEMIA
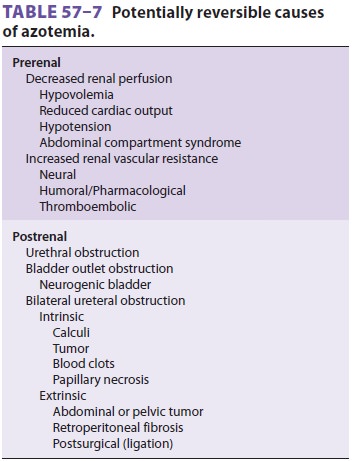
Prerenal azotemia results from hypoperfusion
of the kidneys; if untreated, it progresses to AKI. Renal hypoperfusion
typically the result of decreased arte-rial perfusion pressure, markedly
increased venous pressure, or renal vasoconstriction (Table
57–7). Decreased perfusion pressure is usually
associated with the release of norepinephrine, angiotensin II, and arginine
vasopressin (or antidiuretic hormone). These hormones constrict cutaneous
muscle and splanchnic vasculature and promote salt and water retention. The
synthesis of vasodilating prostaglan-dins (prostacyclin and PGE 2) and nitric oxide in the kidneys and the
intrarenal action of angiotensin II
help maintain glomerular filtration. Use of
cyclo-oxygenase inhibitors (eg, ketorolac for postopera-tive pain control) or
ACE inhibitors in the setting of marked prerenal azotemia can precipitate AKI.
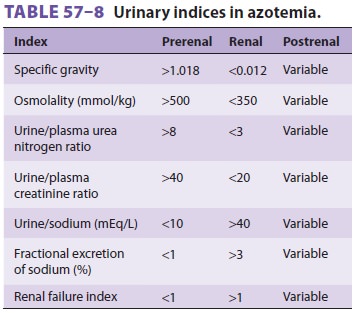
The diagnosis of prerenal azotemia is usually suspected from the clinical
setting and confirmed by urinary laboratory indices (Table
57–8). Treatment of prer-enal azotemia is
directed at correcting intravascular volume deficits, improving cardiac
function, restor-ing a normal blood pressure, and reversing increases in renal
vascular resistance.
Related Topics