Chapter: Clinical Anesthesiology: Perioperative & Critical Care Medicine: Critical Care
Medical Gas Therapy
MEDICAL GAS THERAPY
The therapeutic medical gases include oxygen
at ambient or hyperbaric pressure, helium–oxygen mixtures (heliox), and nitric
oxide. Oxygen is made available in high-pressure cylinders, via pipeline
sys-tems, from oxygen concentrators, as well as in liquid form. Heliox is
occasionally used to partially relieve the increased work of breathing due to
partial upper airway obstruction. Nitric oxide is administered as a direct,
selective pulmonary vasodilator.
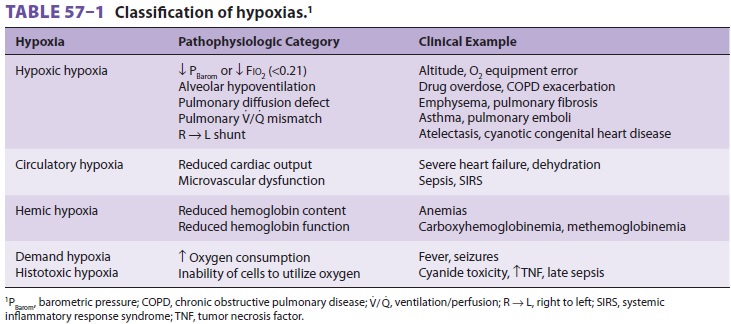
The primary goal of oxygen therapy is to prevent or correct hypoxemia or
tissue hypoxia. Table 57–1 identifies classic categories of
hypoxia.Oxygen therapy alone may not correct either hypoxemia or hypoxia.
Continuous positive airway pressure (CPAP) or positive end-expiratory pres-sure
(PEEP) may be required to recruit collapsed alveoli. Patients with profound
hypercapnia may require ventilatory assistance. High concentrations of oxygen
may be indicated for conditions requir-ing removal of entrapped gas (eg,
nitrogen) from body cavities or vessels. The short-term inhalation of increased
concentrations of oxygen is relatively free of complications.
Supplemental oxygen is
indicated for adults, children, and infants (older than 1 month) when Pao2 is
less than 60 mm Hg (8 kPa) or Sao2 or Spo2 is less than 90% while at rest
breathing room air. In neonates, therapy is recommended if Pao2 is less than 50
mm Hg (6.7 kPa) or Sao2 is less than 88% (or capillary Po2 is less than 40 mm
Hg [5.3 kPa]). Therapy may be indicated for patients when clini-cians suspect
(rather than measure) hypoxemia or hypoxia based on a medical history and physical
examination. Patients with myocardial infarction, cardiogenic pulmonary edema,
acute lung injury, acute respiratory distress syndrome (ARDS), pul-monary
fibrosis, cyanide poisoning, or carbon monoxide inhalation all require
supplemental oxygen. Supplemental oxygen is given during the perioperative
period because general anesthe-sia commonly causes a decrease in Pao2
second-ary to increased pulmonary ventilation/perfusion mismatching and
decreased functional residual capacity (FRC). Supplemental oxygen should be
provided before procedures such as tracheal suc-tioning or bronchoscopy, which
commonly cause arterial desaturation. There is evidence that supple-mental
oxygen is effective in prolonging survival of patients with chronic obstructive
pulmonary disease (COPD) whose resting Pao2 is lower than 60 mm Hg at sea
level. Supplemental oxygen ther-apy also appears to have a mild beneficial
effect on the mean pulmonary arterial pressure and subjec-tive indices of
patients’ dyspnea.
Related Topics