Chapter: Clinical Anesthesiology: Perioperative & Critical Care Medicine: Critical Care
Mechanical Ventilation
MECHANICAL VENTILATION
Despite early intervention and appropriate respi-ratory care, patients
with critical illness will often require mechanical ventilation. Mechanical
venti-lation can replace or supplement normal sponta-neous ventilation. In most
instances, the problem is primarily that of impaired CO2
elimination (ventilatory failure). In other instances, mechani-cal ventilation
may be used as an adjunct (usu-ally to positive-pressure therapy; see) in the
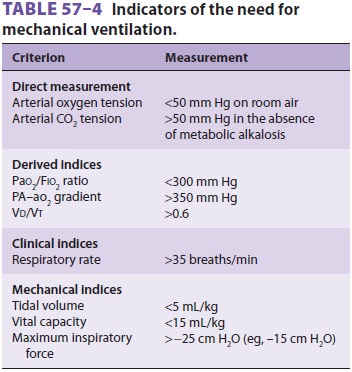
treatment of hypoxemia. The decision to initiate mechanical ventilation is made
on clinical grounds, but certain parameters have been suggested as guidelines (Table
57–4).
Of the two available techniques, positive-pressure ventilation and
negative-pressure ventila-tion, the former has much wider applications and is
almost universally used. Although negative-pressure ventilation does not
require tracheal intubation, it cannot overcome substantial increases in airway
resistance or decreases in pulmonary compliance, and it also limits access to
the patient.
During positive-pressure ventilation, lung
inflation is achieved by periodically applying posi-tive pressure to the upper
airway through a tight-fitting mask (noninvasive mechanical ventilation) or
through a tracheal or tracheostomy tube. Increased airway resistance and
decreased lung compli-ance can be overcome by manipulating inspiratory gas flow
and pressure. The major disadvantages of positive-pressure ventilation are
altered ventila-tion-to-perfusion relationships, potentially adverse
circulatory effects, and risk of pulmonary baro-trauma and volutrauma.
Positive-pressure ventila-tion increases physiological dead space because gas
flow is preferentially directed to the more compli-ant, nondependent areas of
the lungs, whereas blood flow (influenced by gravity) favors dependent areas.
Reductions in cardiac output are primarily due to impaired venous return to the
heart from increased intrathoracic pressure. Barotrauma is closely related to
repetitive high peak inflation pressures and under-lying lung disease, whereas
volutrauma is related to the repetitive collapse and reexpansion of alveoli.
Related Topics