Chapter: Medical Surgical Nursing: Emergency Nursing
Poisoning - Emergency Nursing
Poisoning
A poison is any
substance that, when ingested, inhaled, absorbed, applied to the skin, or
produced within the body in relatively small amounts, injures the body by its
chemical action. Poisoning from inhalation and ingestion of toxic materials,
both intentional and unintentional, constitutes a major health hazard and an
emergency situation. Emergency treatment is initiated with the following goals:
·
To remove or inactivate the
poison before it is absorbed
·
To provide supportive care in
maintaining vital organ systems
·
To administer a specific
antidote to neutralize a specific poison
·
To implement treatment that
hastens the elimination of the absorbed poison
INGESTED (SWALLOWED) POISONS
Swallowed poisons may be corrosive. Corrosive poisons include alkaline and acid agents that can cause
tissue destruction after coming in contact with mucous membranes. Alkaline
products include lye, drain cleaners, toilet bowl cleaners, bleach,
nonphos-phate detergents, oven cleaners, and button batteries (batteries used
to power watches, calculators, or cameras). Acid products include toilet bowl
cleaners, pool cleaners, metal cleaners, rust removers, battery acid.
Management
Control of the airway, ventilation, and oxygenation are
essential. In the absence of cerebral or renal damage, the patient’s progno-sis
depends largely on successful management of respiration and circulation.
Measures are instituted to stabilize cardiovascular and other body functions.
ECG, vital signs, and neurologic status are monitored closely for changes.
Shock, which may result from the cardiodepressant action of the substance
ingested, from venous pooling in lower extremities, or from reduced circulating
blood volume resulting from increased capillary permeability, is treated. An
indwelling urinary catheter is inserted to monitor renal func-tion. Blood
specimens are obtained to test for concentration of drug or poison.
Efforts are initiated to
determine what substance was taken; the amount; time since ingestion; signs and
symptoms, such as pain or burning sensations, any evidence of redness or burn
in the mouth or throat, pain on swallowing or an inability to swallow,
vomiting, or drooling; age and weight of the patient; and pertinent health
history.
Measures are instituted
to remove the toxin or decrease its ab-sorption. The patient who has ingested a
corrosive poison is given water or milk to drink for dilution. However,
dilution is not at-tempted if the patient has acute airway edema or obstruction
or if there is clinical evidence of esophageal, gastric, or intestinal burn or
perforation. The following gastric emptying procedures may be used as
prescribed:
·
Syrup of ipecac to induce
vomiting in the alert patient.
·
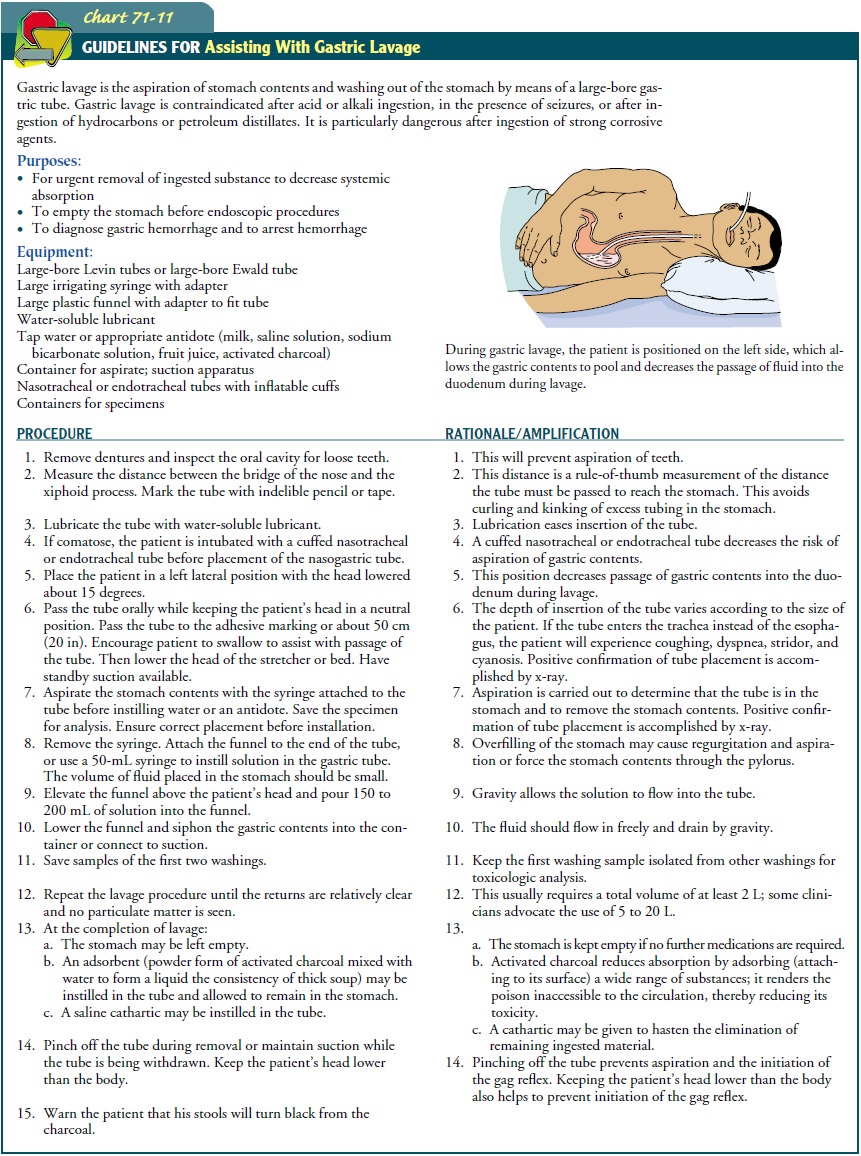
Gastric lavage for the
obtunded patient (Chart 71-11). Gas-tric aspirate is saved and sent to the laboratory
for testing (toxicology screens)
·
Activated charcoal
administration if poison is one that is ab-sorbed by charcoal
·
Cathartic, when appropriate
The specific chemical or
physiologic antagonist (antidote) is administered as early as possible, to
reverse or diminish the effects of the toxin. If these measures are
ineffective, procedures are ini-tiated to remove the ingested substance. These
procedures in-clude administration of multiple doses of charcoal, diuresis (for
substances excreted by the kidneys), dialysis, and hemoperfusion. Hemoperfusion
involves detoxification of the blood by process-ing it through an
extracorporeal circuit and an adsorbent car-tridge containing charcoal or
resin, after which the cleaned blood is returned to the patient.
Throughout
detoxification, the patient’s vital signs, CVP, and fluid and electrolyte
balance are monitored closely. Hypotension and cardiac dysrhythmias are
possible. Seizures are also possible because of CNS excitement from the poison
or from oxygen de-privation. If the patient complains of pain, analgesics are
admin-istered cautiously. Severe pain causes vasomotor collapse and reflex
inhibition of normal physiologic functions.
After the patient’s condition has stabilized and
discharge is im-minent, written material indicating the signs and symptoms of
potential problems related to the poison ingested and signs or symptoms
requiring evaluation by a physician should be given to the patient. If
poisoning was determined to be a suicide attempt, a psychiatric consultation
should be requested before the patient is discharged. In cases of inadvertent
poison ingestion, poison prevention and home poison-proofing instructions
should be provided to the patient and family.
INHALED POISONS: CARBON MONOXIDE POISONING
Carbon monoxide
poisoning may occur as a result of industrial or household incidents or
attempted suicide. It is implicated in more deaths than any other toxin except
alcohol. Carbon monox-ide exerts its toxic effect by binding to circulating
hemoglobin and thereby reducing the oxygen-carrying capacity of the blood.
Hemoglobin absorbs carbon monoxide 200 times more readily than it absorbs
oxygen. Carbon monoxide–bound hemoglobin, called carboxyhemoglobin, does not transport oxygen.
Because the CNS has a critical need for oxygen, CNS symp-toms predominate with carbon monoxide toxicity. A person suffering from carbon monoxide poisoning may appear intoxi-cated (from cerebral hypoxia). Other signs and symptoms include headache, muscular weakness, palpitation, dizziness, and confu-sion, which can progress rapidly to coma. Skin color, which can range from pink or cherry-red to cyanotic and pale, is not a reli-able sign. Pulse oximetry is also not valid, because the haemoglobin is well saturated.
It is
not saturated with oxygen, but the pulse oximeter reads the saturation as such
and presents the false impression that the patient is well oxygenated and in no
danger. Exposure to carbon monoxide requires immediate treatment.
Management
Goals of management are
to reverse cerebral and myocardial hy-poxia and to hasten elimination of carbon
monoxide. Whenever a patient inhales a poison, the following general measures
apply:
·
Carry the patient to fresh air
immediately; open all doors and windows.
·
Loosen all tight clothing.
·
Initiate cardiopulmonary
resuscitation if required; admin-ister oxygen.
·
Prevent chilling; wrap the
patient in blankets.
·
Keep the patient as quiet as
possible.
·
Do not give alcohol in any
form.
In addition, for the
patient with carbon monoxide poisoning, carboxyhemoglobin levels are analyzed
on arrival at the ED and before treatment with oxygen if possible. Then 100%
oxygen is administered at atmospheric or hyperbaric pressures to reverse
hypoxia and accelerate the elimination of carbon monoxide. Oxy-gen is
administered until the carboxyhemoglobin level is less than 5%. The patient is
monitored continuously. Psychoses, spastic paralysis, ataxia, visual
disturbances, and deterioration of mental status and behavior may persist after
resuscitation and may be symptoms of permanent brain damage.
When unintentional
carbon monoxide poisoning occurs, the health department should be contacted, so
that the dwelling or building in question can be inspected. A psychiatric
consultation is warranted if poisoning was determined to be a suicide attempt.
SKIN CONTAMINATION POISONING (CHEMICAL BURNS)
Skin contamination
injuries from exposure to chemicals are chal-lenging because of the large
number of offending agents with diverse actions and metabolic effects. The
severity of a chemical burn is determined by the mechanism of action, the
penetrating strength and concentration, and the amount and duration of exposure
of the skin to the chemical.
Management
The skin should be
drenched immediately with running water from a shower, hose, or faucet.A
constant stream of water should continue as the patient’s clothing is being
removed. The skin of health care personnel as-sisting the patient should be
appropriately protected if the burn is extensive or if the agent is
significantly toxic or is still pres-ent. Prolonged lavage with generous
amounts of tepid water is important.
In the meantime, attempts to determine the identity and
char-acteristics of the chemical agent are necessary for future treat-ment. The
standard burn treatment appropriate for the size and location of the wound
(antimicrobial treatment, débridement, tetanus prophylaxis as prescribed) is
instituted. The patient may require plastic surgery for further wound
management. The pa-tient is instructed to have the affected area reexamined at
24 and 72 hours and in 7 days because of the risk for underestimating the
extent and depth of these types of injuries.
FOOD POISONING
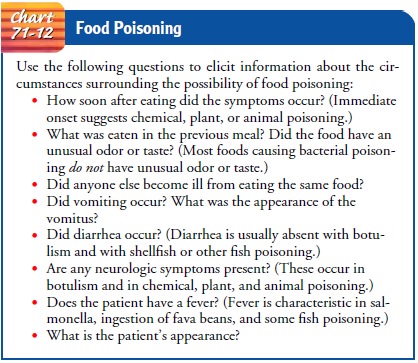
Food poisoning is a sudden illness that occurs after
ingestion of contaminated food or drink. Botulism is a serious form of food
poisoning that requires continual surveillance. See Chart 71-12 for assessment
questions.
Management
The key to treatment is
determining the source and type of food poisoning. If possible, the suspected
food should be brought to the medical facility and a history obtained from the
patient or family.
Food, gastric contents, vomitus, serum, and feces are
collected for examination. The patient’s respirations, blood pressure,
sen-sorium, CVP (if indicated), and muscular activity are monitored closely.
Measures are instituted to support the respiratory system. Death from
respiratory paralysis can occur with botulism, fish poisoning, and other food
poisonings.
Because large volumes of electrolytes and water are lost
by vomiting and diarrhea, fluid and electrolyte balance is also an im-portant
area to assess. Severe vomiting produces alkalosis, and se-vere diarrhea
produces acidosis. Hypovolemic shock may also occur from severe fluid and
electrolyte losses. The patient is as-sessed for signs and symptoms of fluid
and electrolyte imbalances, including lethargy, rapid pulse rate, fever,
oliguria, anuria, hypo-tension, and delirium. Weight and serum electrolyte
levels are obtained for future comparisons.
Measures to control nausea are also important to prevent vom-iting, which could further exacerbate fluid and electrolyte imbal-ances. An antiemetic medication is administered parenterally as prescribed if the patient cannot tolerate fluids or medications by mouth. For mild nausea, the patient is encouraged to take sips of weak tea, carbonated drinks, or tap water. After nausea and vomiting subside, clear liquids are usually prescribed for 12 to 24 hours, and the diet is gradually progressed to a low-residue, bland diet.
Related Topics