Chapter: Clinical Anesthesiology: Anesthetic Management: Pediatric Anesthesia
Pediatric Anesthetic Techniques: Sedation for Procedures in and out of the Operating Room
Sedation for Procedures in and out of the Operating Room
Sedation is often requested for pediatric
patients inside and outside the operating room for nonsur-gical procedures.
Cooperation and motionlessness may be required for imaging studies,
bronchoscopy, gastrointestinal endoscopy, cardiac catheterization, dressing
changes, and minor procedures (eg, cast-ing and bone marrow aspiration).
Requirements vary depending on the patient and the procedure, ranging from
anxiolysis (minimal sedation), to conscious sedation (moderate sedation and
analge-sia), to deep sedation/analgesia, and finally to gen-eral anesthesia.
Anesthesiologists are usually held to the same standards when they provide
moder-ate or deep sedation as when they provide general anesthesia. This
includes preoperative preparation (eg, fasting), assessment, monitoring, and
postop-erative care. Airway obstruction and hypoventila-tion are the most
commonly encountered problems associated with moderate or deep sedation. With
deep sedation and general anesthesia cardiovascular depression can also be a
problem.
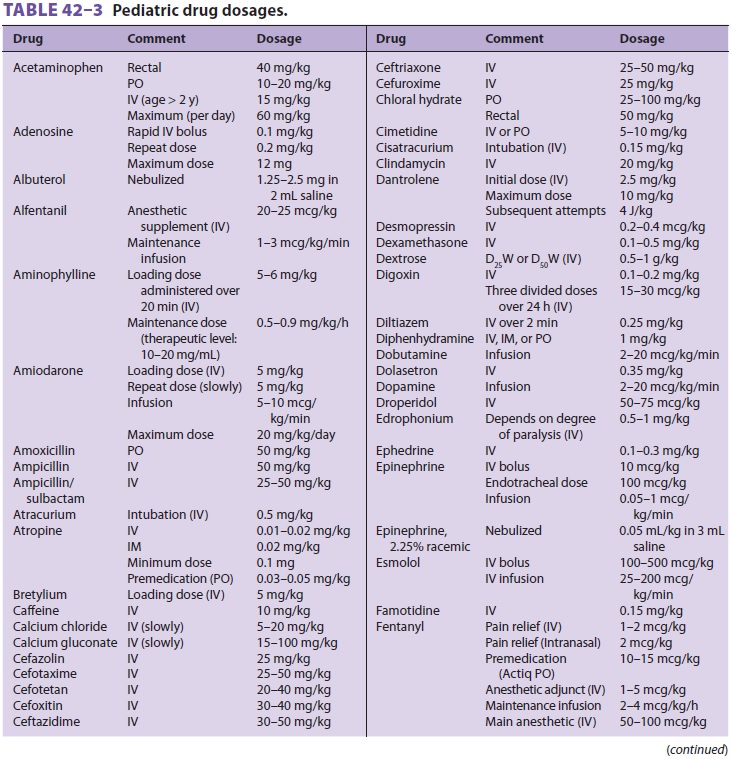
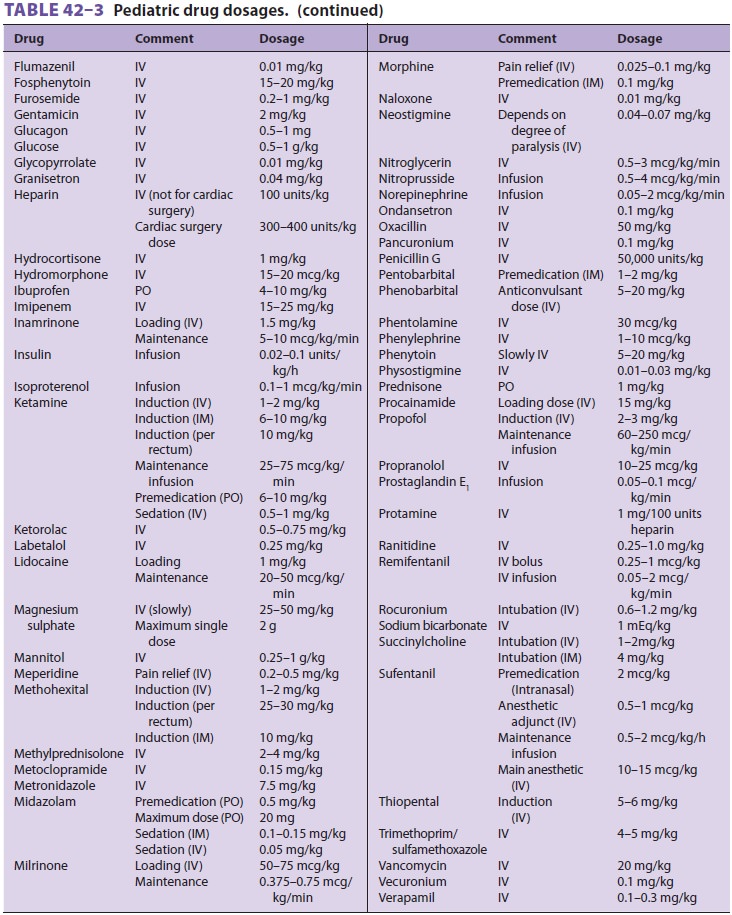
Table 42–3 includes doses of
sedative-hypnotic drugs. One of the sedatives commonly used by non-anesthesia
personnel in the past was chloral hydrate, 25–100 mg/kg orally or rectally. It
has a slow onset of up to 60 min and a long half-life (8–11 h) that results in
prolonged somnolence. Although it generally has little effect on ventilation,
it can cause fatal airway obstruction in patients with sleep apnea. Overall,
chloral hydrate is a poor choice given its propensity for producing cardiac
arrhythmias when it is used in the larger doses needed for moderate sedation.
Midazolam, 0.5 mg/kg orally or 0.1–0.15 mg/kg intravenously, is particularly useful
because its effects can be readily reversed with flumazenil. Doses should be
reduced whenever more than one agent is used because of the potential for
synergistic respira-tory and cardiovascular depression.Propofol is by far the
most useful sedative-hypnotic drug. Although the drug is not approved for
sedation of pediatric ICU patients and is not approved for administration by
anyone other than those trained in the administration of general anes-thesia,
it can be dosed safely for most procedures at infusion rates up to 200
mcg/kg/min. In coun-tries other than the United States, propofol is often
administered using the Diprifusor, a computer-controlled infusion pump that
maintains a constant target site concentration. Supplemental oxygen and close
monitoring of the airway, ventilation, and other vital signs are mandatory (as
with other agents). An LMA is usually well tolerated at higher doses.
Related Topics