Chapter: Clinical Anesthesiology: Anesthetic Management: Pediatric Anesthesia
Anesthetic Considerations in Tracheoesophageal Fistula
TRACHEOESOPHAGEAL FISTULA
Pathophysiology
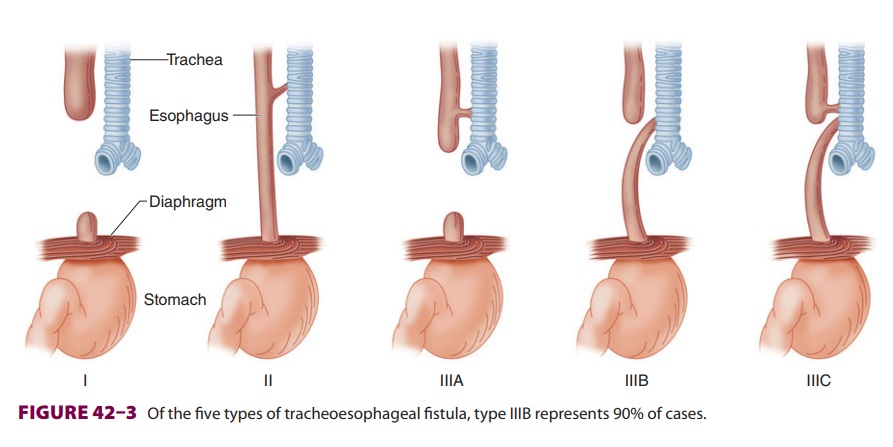
There are several types of tracheoesophageal fistula (Figure
42–3). The
most common (type IIIB) is the combination of an upper esophagus that ends in a
blind pouch and a lower esophagus that connects to
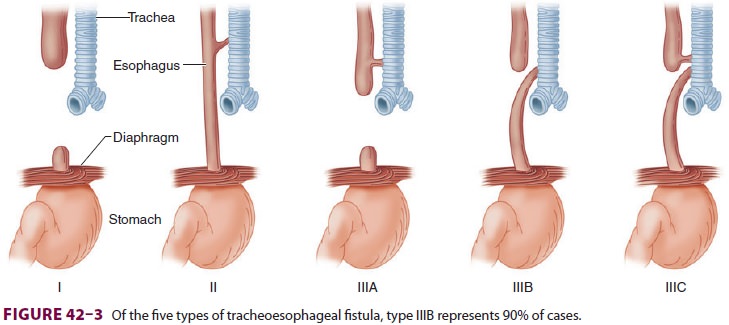
the trachea. Breathing results in gastric
distention, whereas feeding leads to choking, coughing, and cyanosis (three
Cs). The diagnosis is suspected by failure to pass a catheter into the stomach
and con-firmed by visualization of the catheter coiled in a blind, upper
esophageal pouch. Aspiration pneumo-nia and the coexistence of other congenital
anoma-lies (eg, cardiac) are common. These may include the association of
vertebral defects, anal atresia, tracheoesophageal fistula with esophageal
atresia, and radial dysplasia, known as the VATER syn-drome. The VACTERL
variant also includes cardiac and limb anomalies. Preoperative management is
directed at identifying all congenital anomalies and preventing aspiration
pneumonia. This may include maintaining the patient in a head-up position,
using an oral-esophageal tube, and avoiding feedings. In some instances
gastrostomy may be performed under local anesthesia. Definitive surgical
treatment is usually postponed until any pneumonia clears or improves with
antibiotic therapy.
Anesthetic Considerations
These neonates tend to have copious pharyngeal secretions that require
frequent suctioning before and during surgery. Positive-pressure ventilation is
avoided prior to intubation, as the resulting gas-tric distention may interfere
with lung expansion. Intubation is often performed awake and without muscle
relaxants. These neonates are often dehy-drated and malnourished due to poor
oral intake.
The key to successful management is correct
endotracheal tube position. Ideally, the tip of the tube lies distal to the
fistula and proximal to the carina, so that anesthetic gases pass into the
lungs instead of the stomach. This is impossible if the fis-tula connects to
the carina or a mainstem bronchus. In these situations, intermittent venting of
a gastros-tomy tube may permit positive-pressure ventilation without excessive
gastric distention. Suctioning of the gastrostomy tube and upper esophageal pouch
tube helps prevent aspiration pneumonia. Surgical division of the fistula and
esophageal anastomosis is performed via a right extrapleural thoracotomy with
the patient in the left lateral position. A precordial stethoscope should be
placed in the dependent (left) axilla, since obstruction of the mainstem
bronchus during surgical retraction is not uncommon. A drop in oxygen
saturation indicates that the retracted lung needs to be reexpanded. Surgical
retraction can also compress the great vessels, trachea, heart, and vagus
nerve. Blood pressure should be continu-ously monitored with an arterial line.
These infants often require ventilation with 100% oxygen. Blood should be
immediately available for transfusion. Postoperative complications include
gastroesopha-geal reflux, aspiration pneumonia, tracheal com-pression, and
anastomotic leakage. Most patients must remain intubated and receive
positive-pressure ventilation in the immediate postoperative period. Neck
extension and instrumentation (eg, suction-ing) of the esophagus may disrupt
the surgical repair and should be avoided.
Related Topics