Chapter: Basic & Clinical Pharmacology : General Anesthetics
Intravenous Anesthetics
INTRAVENOUS
ANESTHETICS
Intravenous
nonopioid anesthetics play an important role in the practice of modern
anesthesia. They are widely used to facilitate rapid induction of anesthesia
and have replaced inhalation as the preferred method of anesthesia induction in
most settings except for pediatric anesthesia. Intravenous agents are also
commonly used to provide sedation during monitored anesthesia care and for
patients in intensive care (ICU) settings. With the introduction of propofol,
intravenous anesthesia also became an option for the maintenance of anesthesia.
However, similar to the inhaled agents, the currently avail-able intravenous
anesthetics are not ideal anesthetic drugs in the sense of producing all and
only the five desired effects (unconsciousness, amnesia, analgesia, inhibition
of autonomic reflexes, and skeletal muscle relaxation). Therefore, balanced anesthesia with multiple drugs
(inhaled anesthetics, sedative-hypnotics, opioids, neuromuscular blocking
drugs) is generally used to minimize unwanted side effects.
The
intravenous anesthetics used for induction of general anes-thesia are
lipophilic and preferentially partition into highly per-fused lipophilic
tissues (brain, spinal cord), which accounts for their rapid onset of action.
Regardless of the extent and speed of their metabolism, termination of the
effect of a single bolus is determined by redistribution of the drug into less
perfused and inactive tissues such as skeletal muscle and fat. Thus, all drugs
used for induction of anesthesia have a similar duration of action when
administered as a single bolus dose despite significant differences in their
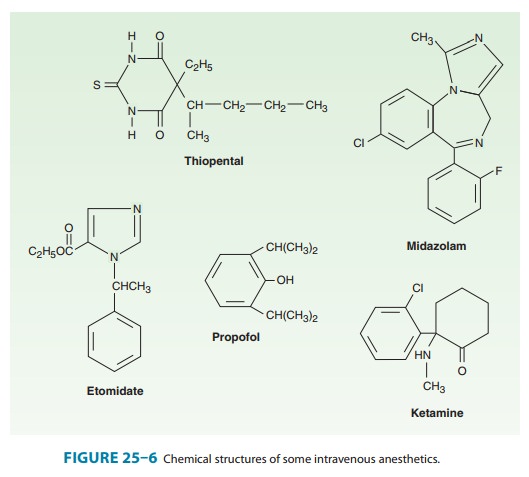
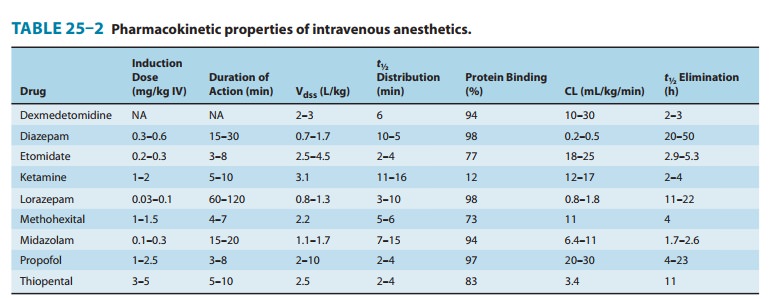
metabolism. Figure 25–6 shows the chemical structures of common clinically used
intravenous anesthetics. Table 25–2 lists pharmacokinetic properties of these
and other intravenous agents.
Related Topics