Chapter: Basic Radiology : Radiology of the Chest
Exercise: The Opaque Hemithorax
EXERCISE 4-1.
THE OPAQUE HEMITHORAX
4-1. The most likely
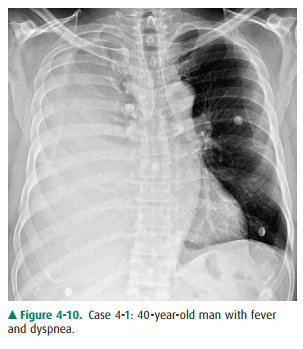
diagnosis for Case 4-1 (Figure 4-10) is
A.
massive right pleural effusion.
B.
total atelectasis of the right lung.
C.
left pneumothorax.
D.
aplasia of the right lung.
E.
mediastinal hematoma.
4-2. The most likely
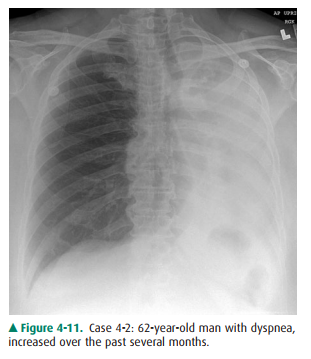
diagnosis for Case 4-2 (Figure 4-11) is
A.
left pleural effusion.
B.
collapse of the left lung.
C.
right pneumothorax.
D.
collapse of the right lung.
E.
mediastinal hematoma.
Radiologic Findings
4-1. In this case, a
frontal chest radiograph (Figure 4-10) shows that the right hemithorax is
opaque. Signs of mass effect are present and suggest a space-occupying lesion
in the right hemithorax. There is shift of the mediastinum toward the contralateral hemithorax, as evidenced
by shift of the trachea and left heart border to the left. If a nasogastric
tube were in place, esophageal shift could be inferred from the shift of the
nasogastric tube. Space-occupying lesions also cause inferior displacement of
the hemidiaphragm. Although the diaphragm itself is not visible, when the
process is on the left, one can infer that the di-aphragm is depressed by the
inferior displacement of the gastric air bubble. Mass effect may also widen the
distance between ribs. In this patient, the space-occupying lesion was a large
right pleural effusion resulting from tuberculous empyema. A chest CT scan
(Figure 4-12) in this patient shows the large pleural effusion and complete
collapse of the underlying right lung against the medial aspect of the right
hemithorax (A is the correct answer to Question 4-1).
4-2. In this case, a
frontal chest radiograph (Figure 4-11) shows that the left hemithorax is
opaque. In con-trast to the patient in Figure 4-10, the patient in Figure 4-11 has
signs of volume loss within the left hemithorax. There is mediastinal shift
toward the ipsilateral hemithorax, as
evidenced by shift of the trachea and
the right heart border into the left hemithorax. The gastric air bubble is
higher in the left upper quadrant of the abdomen than is nor-mally seen,
because of elevation of the left hemidi-aphragm. The mediastinal window of the
chest CT examination (Figure 4-13A) shows the mediastinal shift to the left and
consolidation of the left lung. The lung window of the chest CT examination
(Figure 4-13B) shows that the right lung is aerated. In this patient, the left
lung collapse is due to a bronchogenic carcinoma in the left main bronchus
(asterisk). This case exhibits the signs of volume loss, as opposed to mass
effect (B is the correct answer to Question 4-2).
Discussion
This exercise reviews the
principal signs that allow one to distinguish mass effect from volume loss. The
mass effect caused by a tumor or by a large pleural effusion expands the
hemithorax and displaces the trachea, mediastinum, and diaphragm away from the
mass. There may be a subtle in-crease in the distance between ribs. Volume
loss, on the other hand, decreases the size of the hemithorax, and the trachea,
mediastinum, and diaphragm move toward the involved hemithorax. The distance
between the ribs on the abnormal side will be slightly decreased. In Figure
4-10, the opacifica-tion of the right hemithorax occurs as a result of massive
right pleural effusion, and the right lung is collapsed as a re-sult of both
compression by the fluid present within the right pleural space and a loss of
the negative intrapleural pressure that keeps the lung in close juxtaposition
to the chest wall. In Figure 4-11, the collapse is due to obstruction of the left
main bronchus, resulting in atelectasis (airless-ness) of the left lung.
Related Topics