Chapter: Basic Radiology : Radiology of the Chest
Exercise: Pleural Abnormalities
EXERCISE 4-12.
PLEURAL ABNORMALITIES
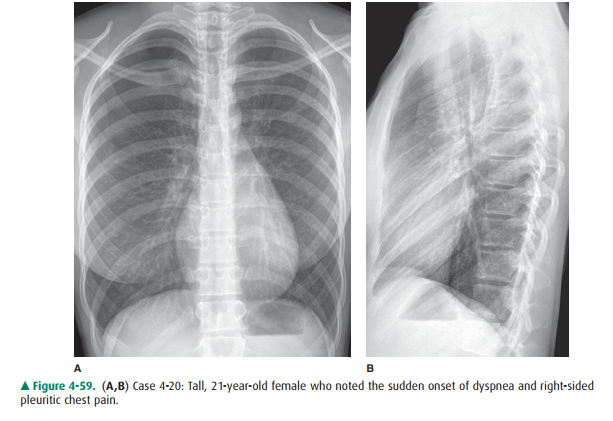
4-20. The most likely
diagnosis in Case 4-20 (Figure 4-59 A,B) is
A.
pulmonary embolism.
B.
overinflation associated with asthma.
C.
pneumothorax.
D.
normal chest, with a skin fold projected over the right
hemithorax.
E.
left lower lobe atelectasis.
Radiologic Findings
4-10. In Figure 4-59,
there is increased radiolucency in the periphery of the right hemithorax. On
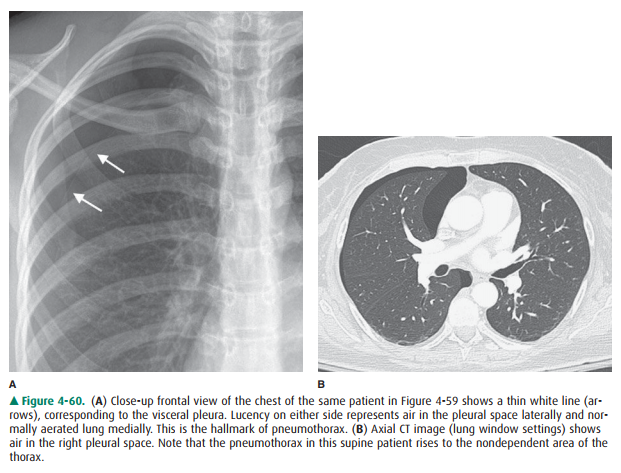
the close-up of the right lung (Figure 4-60 A), there is a thin white line
(arrows) paralleling, but displaced from, the right lateral chest wall. The
thin line represents the visceral pleura. There is air-filled lung medial to
this thin white line, and there is air within the pleural space lateral to this
line. Note the absence of pul-monary vessels lateral to the pleural line (C is
the cor-rect answer to Question 4-20).
Discussion
Pneumothorax is the presence of
air in the pleural space. The lung collapses away from the chest wall because
of its normalelastic recoil. In some instances, a ball valve mechanism is
present, and air continues to enter the pleural space and further collapses the
lung and displaces the mediastinum away from the side of the pneumothorax. The
relationship of the air in the pleural space to the lung and chest wall can be clearly
seen on the CT scan of a patient with a right pneumothorax (Figure 4-60 B).
Note that air rises to the highest point in the thorax, the anterior thorax in
a supine patient and the lung apex in an upright patient. The visceral pleura
covering the lung is visible as a thin white line on both chest radiographs and
CT scans. No pulmonary vessels may be seen extending beyond the pleural line,
and the air in the pleural space appears more radiolucent than the ad-jacent
lung.
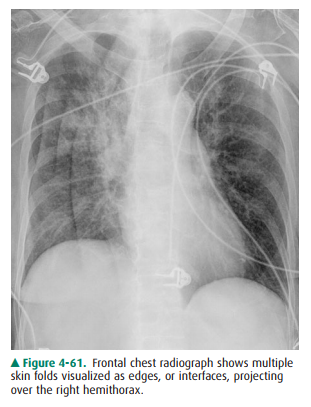
The most common mimic of a
pneumothorax, particu-larly in a supine patient, is a skin fold. The image
receptor for portable AP chest radiographs is placed behind the pa-tient’s
back. Skin folds may be pressed between the pa-tient’s back and the receptor.
Radiographically, a skin fold produces an interface, or an edge of thick tissue
outlined by the greater radiolucency of the superimposed lung (Figure 4-61). If
you can distinguish an edge from a line, then you can distinguish a skin fold
from a pneumothorax. The ab-sence of pulmonary markings beyond the pleural line
is supporting evidence for a pneumothorax. Because the vessels taper as they
approach the lung periphery, the ves-sels in the extreme periphery of the lung
may be too tiny to see.
Pneumothorax is considered
spontaneous if it occurs in the absence of trauma (including barotrauma).
Sponta-neous pneumothorax may be primary and occur in the ab-sence of
significant other lung disease, or it may occur secondarily because of lung
disease. Apical blebs are present in a high percentage of patients with primary
sponta-neous pneumothorax, and their rupture is thought to be the most frequent
cause of spontaneous pneumothorax. For unknown reasons, it occurs most frequently
in tall young men. Secondary spontaneous pneumothorax may occur in association
with any cavitary lesion that lies in the periphery of the lung, as well as in
emphysema, in bullous disease, and in pulmonary fibrosis of a variety of
etiologies.
Related Topics