Chapter: Basic Radiology : Radiology of the Chest
Exercise: Lobar Atelectasis
EXERCISE 4-2.
LOBAR ATELECTASIS
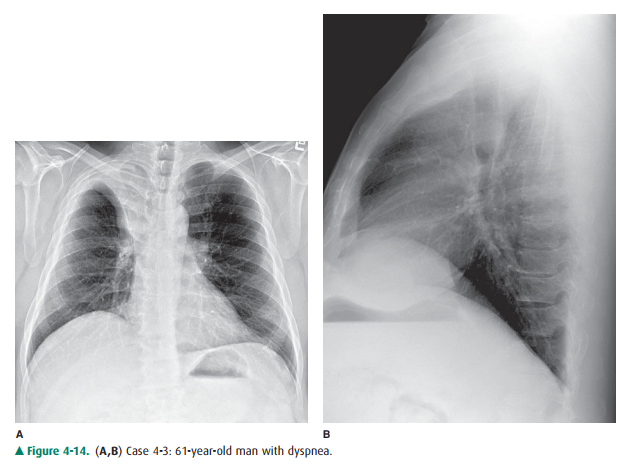
4-3. In Figure 4-14 A,B,
the inferior margin of the opacity in the right upper thorax is due to
A.
the major fissure in right upper lobe (RUL) col-lapse without a
hilar mass.
B.
the minor fissure in RUL collapse with a hilar mass.
C.
the minor fissure in RUL collapse without a hilar mass.
D.
the major fissure in RUL collapse with a hilar mass.
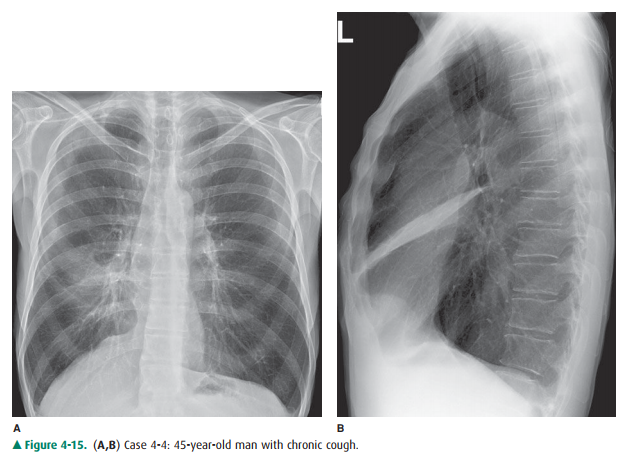
4-4. In Figure 4-15 A,B,
which of the following is true re-garding right middle lobe collapse?
A.
A triangular opacity is superimposed on the heart on the frontal
radiograph.
B.
The right heart border is obscured.
C.
The minor fissure is superiorly displaced.
D.
The right heart border is shifted to the left.
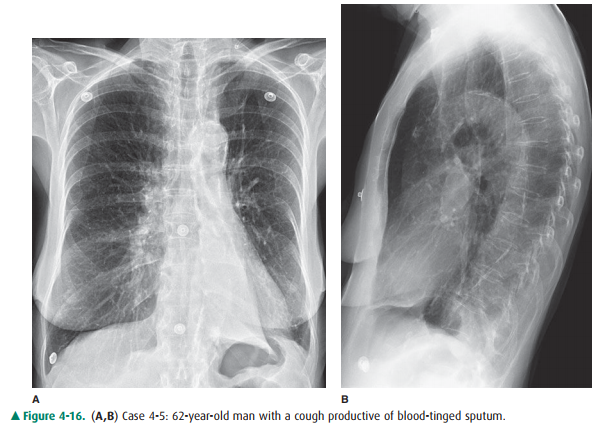
4-5. In Figure 4-16 A,B,
a sign of left lower lobe collapse in this patient is which of the following?
A.
Obscuration of the lateral wall of the ascending thoracic aorta
B.
Superior displacement of the left hilum
C.
Obliteration of the anterior aspect of the left hemidiaphragm on
the lateral view
D.
Triangular opacity in the left retrocardiac area on the frontal
view
E.
Shift of the major fissure toward the anterior chest wall on the
lateral view
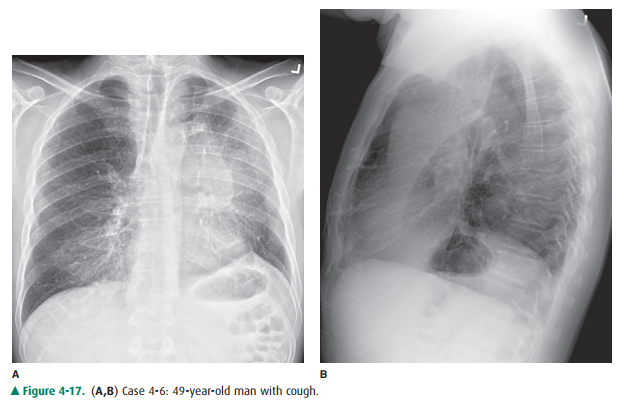
4-6. In Figure 4-17 A,B,
signs of left upper lobe collapse seen in this patient include which of the
following?
A.
Crescent of air around the transverse section of the aortic arch
resulting from hyperexpansion of the superior segment of the left lower lobe
B.
Posterior displacement of the left major fissure on the lateral
view
C.
Obscuration of the right heart border
D.
Tracheal deviation to the right
E.
Inferior displacement of the left hilum.
Radiologic Findings
4-3. In Figure 4-14,
there is opacity in the right upper lung that is sharply marginated on its
inferior border. Vol-ume loss is evidenced by the slight displacement of the
trachea into the right hemithorax, the position of the right heart border
further to the right of the thoracic spine than normal, and the slight
elevation of the right hemidiaphragm, which is normally 1 to 1.5 cm higher than
the left hemithorax. The pulmonary vessels of the right hilum are obscured by
opacity in the right upper thorax. The configuration of the inferior margin of
the opacity is that of a reverse S or S on its side. The “S-sign of Golden”
describes the appearance of the minor fis-sure in right upper lobe collapse,
which is due to bron-chogenic carcinoma. In this case, bulky right hilar
lymph-node enlargement has caused extrinsic com-pression of the right upper
lobe bronchus and has re-sulted in right upper lobe collapse. The right hilar
mass tethers the medial aspect of the minor fissure toits normal midthoracic
position, whereas the lateral aspect of the minor fissure moves freely and
collapses superiorly. In patients in whom the minor fissure is in-complete,
collateral air drift across the canals of Lam-bert and the pores of Kohn may
allow a lobe to remain aerated despite complete obstruction of its bronchus. In
Figure 4-14 A, hyperexpansion of the superior seg-ment of the right lower lobe
produces the ovoid lu-cency on the medial aspect of the collapsed right upper
lobe. On the lateral radiograph, a V-shaped opacity is seen at the lung apex. A
mass-like opacity is superim-posed on the suprahilar area, corresponding to a
com-bination of tumor and atelectatic lung (B is the correct answer to Question
4-3). In patients with right upper lobe collapse without a hilar mass, the
fissure is able to rotate in a straighter line and does not result in the
re-verse S sign. The major fissure is oriented in a coronal plane and is not
normally visualized on the frontal chest radiograph. Therefore, the major
fissure would not account for the opacity seen on the frontal chest radiograph,
either with or without a hilar mass.
4-4. In Figure 4-15 A,B, the right
heart border is obscuredby adjacent opacity on the PA radiograph. The lungs are
hyperinflated. The heart is in the midthorax in approximately its normal
position. The heart border has not been displaced to the left. On the lateral
radiograph, a narrow triangular opacity is superimposed on the heart. The apex
of the triangle points toward the hilum, and the base of the triangle is
against the anterior chest wall. This is a collapsed right middle lobe. The
right hemidiaphragm is slightly elevated, but there are no other signs of
significant volume loss. Right middle lobe collapse may have minimal impact on
the overall volume in the right hemithorax because it is the smallest of the
pulmonary lobes, and the upper and lower lobes can expand to compensate for its
volume loss. Right middle lobe collapse, unlike other lobar collapse, is often
due to benign causes, such as extrinsic pressure by enlarged lymph nodes, which
totally surround the bronchus. This enlarge ment is most frequently due to
granulomatous disease of an infectious or noninfectious nature (B is the
correct answer to Question 4-4).
4-5. When the left lower lobe
collapses, the result is a triangular opacity, which can be quite subtle,
behind the heart. Secondary signs of volume loss, however, should prompt one to
look closely for the collapse. These signs include shift of the trachea and
heart to the left (note that the right heart border is now superimposed on the
thoracic spine), inferior displacement of the left hilum,and elevation of the
left hemidiaphragm. On the lateral radiograph, the right hemidiaphragm is
visible along its entire contour. However, the left hemidiaphragm is obscured
posteriorly because it is “silhouetted” by the collapsed left lower lobe.
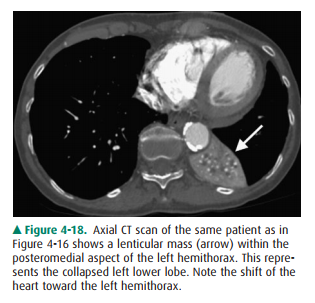
Because it is tethered medially by the inferior pulmonary ligament, the left
lower lobe collapses posteriorly and medially (Figure 4-18). The major fissure
is displaced posteriorly, as well as
rotated into a more sagittal orientation than the normal coronal orientation (D
is the correct answer to Question 4-5). You may have noted the large lung volumes in this patient, which are due to centrilobular
emphysema. In this patient, who has a long history of cigarette smoking, a
squamous-cell carcinoma in the left lower lobe bronchus was responsible for the
collapsed left lower lobe. he primary sign of volume loss in Figure 4-17 B is
anterior displacement of the left major fissure on the lateral radiograph.he
collapsed left upper
lobe is opaque as a result of
both airlessness and postobstructive pneumonitis. When there is little
neumonitiswithin the obstructed lobe, the left upper lobe can collapse
completely behind the anterior chest wall, so that only a narrow band of
opacity is visible behind the sternum. In this situation, the diagnosis may be
suggested by the secondary signs of volume loss. Note the shift of the trachea
to the left and the slight elevation of the left hemidiaphragm. The left lower
lobe is hyperexpanded.The hyperexpanded superior segment of the left lower lobe
produces a crescent of air around the transverse section of the aortic arch on
the PA radiograph. A thin opaque line is visible at the apex of the left
hemidi-aphragm on the PA radiograph. Presence of this line, called a
juxtaphrenic peak, should prompt one to look for upper lobe collapse. The hilum
may be displaced anteriorly in left upper lobe collapse, but it is never
dis-placed inferiorly. Option E, inferior displacement of the left hilum, is
therefore false (A is the correct answer to Question 4-6). Because the lingular
bronchus arises from the left upper lobe bronchus, the lingular seg-ment of the
left upper lobe is collapsed as well in this patient. The lingula is adjacent
to the left heart border and is responsible for the obscuration of the left
heart border in left upper lobe collapse.
Discussion
The term atelectasis refers to volume loss, or airlessness, within the lung.
The term collapse is often used to
describe complete atelectasis of an entire lobe or an entire lung. Atelectasis
can occur as a result of several pathophysiologic processes. Ob-struction of a
bronchus by bronchogenic carcinoma should al-ways be considered in an adult with
lobar atelectasis. The tumor may be within the bronchus (endobronchial), as
occurs with squamous-cell carcinoma or small-cell undifferentiated carcinoma.
The tumor may be outside the bronchus, and en-larged lymph nodes may cause
extrinsic compression of the bronchus. In a child, aspiration of a foreign body
is a more likely cause of obstruction of a bronchus. Complete obstruc-tion of a
lobar bronchus may not always result in lobar collapse because pathways of
collateral ventilation are present within the lung. The pores of Kohn and the
canals of Lambert allow collateral air drift between adjacent areas of lung but
do not ex-tend across pleural surfaces. The visceral pleural surface that
covers the lung creates the interlobar fissures (minor fissure, major fissure)
that separate lobes of the lungs. These fissures are not always complete,
however, and may not extend entirely across the lung. When the right upper lobe
bronchus is oc-cluded, for example, the right upper lobe may remain partially
aerated as a result of collateral air drift from the right middle lobe, around
an incomplete minor fissure. Obstruction of smaller airways can occur as a
result of mucous plugs, which are often present in intubated patients and in
patients with chronic small airway disease.
Passive atelectasis (see Figure
4-10) occurs as a result of a space-occupying process within the pleural space.
This is also called relaxation atelectasis, because the lung is no longer
ex-posed to the negative intrapleural pressure that normally keeps the lung
apposed to the chest wall. Any space-occupying pleural process, including a
large pneumothorax (air in the pleural space), pleural effusion, hemothorax
(blood in the pleural space), or pleural tumor, can cause atelectasis within
the underlying lung. Compressive
atelectasis is the term used to describe atelectasis caused by a
space-occupying process within the lung itself. Cicatrization atelectasis describes the volume loss that occurs as
a result of pulmonary scarring. Adhesive
atelectasis occurs when there is a loss of the pul-monary surfactant that
maintains the surface tension that keeps alveoli open. Adhesive atelectasis
occurs with pul-monary embolism, and with respiratory distress syndrome of the
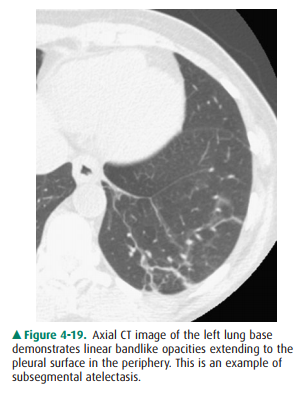
newborn. Atelectasis of small areas of lung is often referred to as subsegmental atelectasis and may be
recog-nized as linear bands of opacity, often at the lung bases (Figure 4-19).
It is helpful to remember the
normal positions of the hemidiaphragms, trachea, mediastinum, and hila so that
displacement of these structures can be readily noted. In most patients, the
left hilum appears slightly higher than the right, because the left hilar
opacity is predominantly due to the left pulmonary artery arching over the left
main bronchus. The right hemidiaphragm is usually 1.0 to 1.5 cm higher than the
left hemidiaphragm. The trachea should be in the midline, and the spinous
processes of the upper tho-racic vertebrae should be superimposed on the center
of the tracheal air column. The right heart border normally lies just to the
right of the thoracic spine. Subtle signs of volume loss may be more readily
appreciated by compari-son of the patient’s radiograph with baseline
radiographs taken previously.
Related Topics