Chapter: Basic Radiology : Radiology of the Chest
Exercise: Occupational Disorders
EXERCISE 4-10.
OCCUPATIONAL DISORDERS
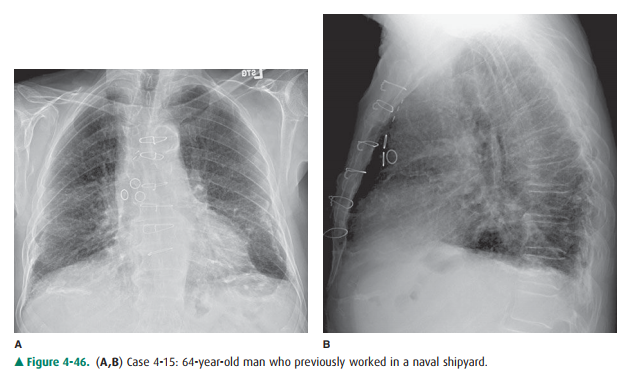
4-15. The most likely
diagnosis in Figure 4-46 A,B is
A.
progressive massive fibrosis, due to silicosis.
B.
pneumonia in a patient with chronic interstitial lung disease.
C.
lung cancer in a patient with asbestosis.
D.
rounded atelectasis in a patient with asbestosis.
E.
calcified plaques in a patient with asbestos exposure.
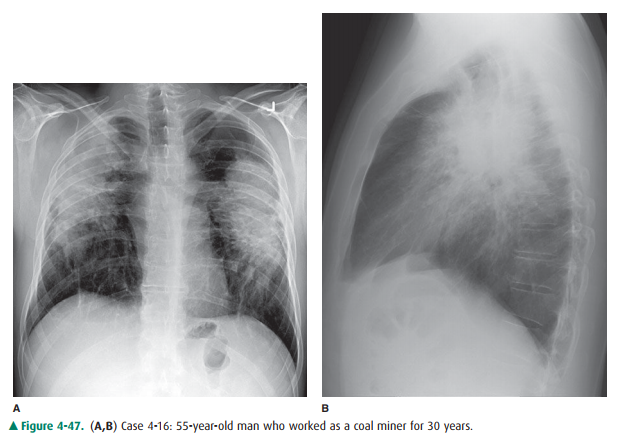
4-16. The most likely
diagnosis in Figure 4-47 A,B is
A.
progressive massive fibrosis, due to silicosis.
B.
pneumonia in a patient with chronic interstitial lung disease.
C.
lung cancer in a patient with asbestosis.
D.
rounded atelectasis in a patient with asbestosis.
E.
calcified plaques in a patient with asbestos exposure.
Radiologic Findings
4-15. The dense
radiopaque lines projecting adjacent to both diaphragmatic surfaces on the PA
and lateral radiographs represent calcified pleural plaques. These are better
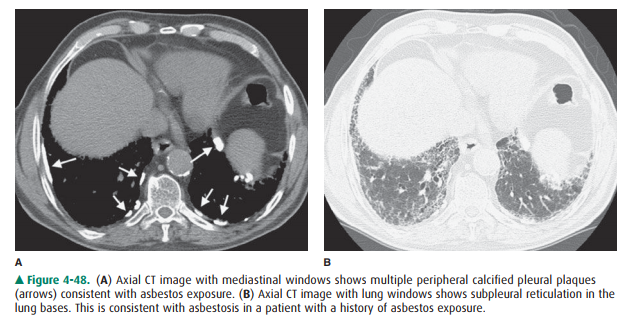
seen on the CT (Figure 4-48 A). When the pleural plaques are seen en face on
the PA radiograph, they produce irregular opacities over the lung. These
opacities have been describedas having a holly leaf appearance. At the lung
bases, a network of fine lines is superimposed over the normal vascular
shadows. These subpleural reticu-lar markings represent interstitial pulmonary
fibro-sis, which almost certainly represents asbestosis (Figure 4-48 B). (E is
the correct answer to Ques-tion 4-15.)
4-16. The patient in Figures
4-47 A,B has two large opaci-ties projecting over the upper lung zones
bilaterally. Bilateral upper lobe volume loss is indicated by up-ward
displacement of the hila. Nodular diseases that have an upper-lobe
preponderance include silicosis, sarcoidosis, and eosinophilic granuloma. In
this case, the nodules have coalesced into large masses, an en-tity known as
progressive massive fibrosis. In this pa-tient with a history of working in
coal mines, the most likely of these diseases is silicosis, or coal worker’s
pneumoconiosis (A is the correct answer to Question 4-16).
Discussion
The two most commonly encountered
occupational lung dis-eases in the United States are asbestosis and silicosis.
Devel-opment of these diseases is dose dependent, and there is alatent period
of many years between exposure and disease. Asbestos-related diseases occur
after exposure to asbestos particles, which are found in many types of
insulation, fire-proofing materials, concrete, and brake linings. The patient
with asbestos exposure is at an increased risk of developing lung cancer. If
the patient also smokes, there is an additive risk, and these patients may be
as much as 100 times more likely to develop lung cancer than the nonsmoking
individual with no asbestos exposure.
The term asbestosis is used to refer to the pulmonary fi-brosis that may be
incited by the presence of the mineral and is not used in reference to the
pleural disease. The pul-monary fibrosis is predominantly distributed in the
lung bases. When severe, it is detected with conventional chest radiography.
When it is more subtle, CT is required for its demonstration (see Figure 4-48
B). When the abnormali-ties are confined to the pleura, the process is called
as-bestos-related pleural disease. There are five manifestations of
asbestos-related pleural disease: asbestos-related pleural effusion, diffuse
pleural thickening, pleural plaques, rounded atelectasis, and malignant
mesothelioma. As-bestos-related pleural effusion occurs from 7 to 15 years
after exposure. It is self-limited and may resolve without sequelae or result
in diffuse pleural thickening. Pleural plaques are fibrous plaques that occur
predominately onthe parietal pleural surfaces of the lower thoracic wall and
diaphragmatic surfaces. Pleural plaques may be up to 8 to 10 mm thick, but are
not easily visualized when seen en face. Oblique radiographs may show plaques
that are pro-jected en face on the PA chest radiograph. The plaques usu-ally
occur 10 years or more after exposure. Early in the development of pleural
disease, the plaques are not calci-fied, but with time, the incidence of
calcification increases. CT is the most sensitive method of identifying pleural
plaques (see Figure 4-48 A). Diffuse pleural thickening may result from the
scarring of a previous benign asbestos-related pleural effusion, or it
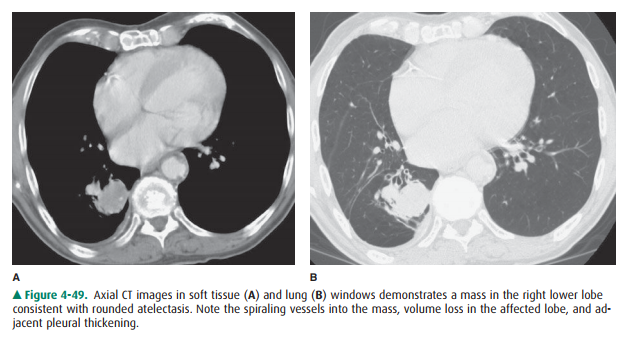
sometimes is due to confluent pleural plaques. Rounded atelectasis (Figures
4-49 A,B) is a piece of folded lung tissue that appears as a mass adjacent to
the chest wall. The parietal pleura adheres to an area of lung, usually in the
posterior lower lobes, and gradually produces a spiraling folded area of lung,
which mimics lung cancer. The comet-tail appearance of bronchi and ves-sels
spiraling into the mass may suggest the correct diagno-sis, but because there
is such a great increase in the risk of lung cancer in the asbestos-exposed
individual, the mass should be closely followed. PET scans and biopsy may be
necessary to distinguish the mass of rounded atelectasis from lung cancer. The
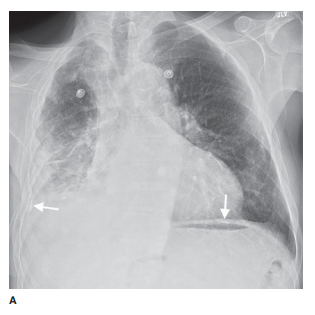
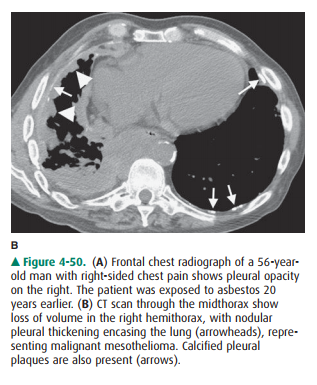
final asbestos-related disease of the pleura is malignant mesothelioma. This is
a malignant tumor of the pleura that usually presents as pleural nod-ules or
pleural effusion (Figure 4-50 A,B).
Silicosis is another form of
pulmonary fibrosis that oc-curs after prolonged exposure to silica.
Historically, it hasmost often developed in coal miners. Because of improved
ventilation standards and the increased automation of coal mining, silicosis is
less commonly encountered today. There is an increased incidence of
tuberculosis in coal min-ers, but no increased risk of lung cancer has been
reported. Because of particle deposition, silicosis is predominantly an
upper-lobe process. It first appears as small pulmonary nodules, and as the
fibrosis progresses the hila are retracted upward over a period of years. The
small granulomatous nodules of simple silicosis coalesce to form larger
con-glomerate masses. When these reach at least 1 cm in diam-eter, the disease is
called complicated silicosis, and as they become larger still, it is designated
progressive massive fi-brosis. Very early disease may be seen only on CT,
although in the later stages of the process, the small nodules and conglomerate
masses are readily seen on either conven-tional radiographs or CT images (see
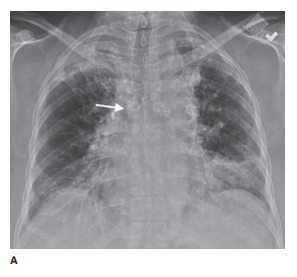
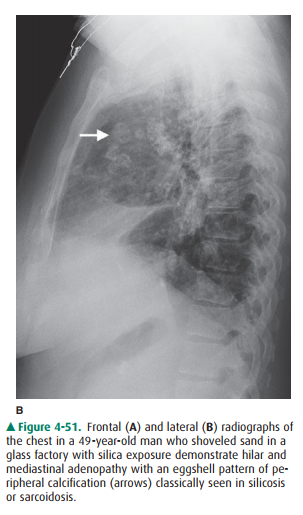
Figure 4-47 A,B). Hilar and mediastinal lymph nodes may calcify in the
pe-riphery of the lymph node, a type of calcification known as eggshell
calcification (Figure 4-51 A,B). An acute form of silicosis can occur in
sandblasters who inhale a massive amount of sand. This type of silicosis
radiographically re-sembles pulmonary edema. Coal worker’s pneumoconiosis is a
similar process that results from inhalation of coal of a relatively pure
carbon content. This dust is relatively more inert than silica and incites less
fibrosis. The nodules are less well defined on their periphery, and there is a
lesser tendency to develop progressive massive fibrosis. These distinctions are
rather artificial, as rock dust is usually not very pure and contains a mixture
of silica, carbon, and other minerals.
Related Topics