Chapter: Basic Radiology : Radiology of the Chest
Exercise: Airspace Diseases
EXERCISE 4-3. AIRSPACE DISEASES
4-7. Which of the following is the best descriptor of Figure4-20 A,B?
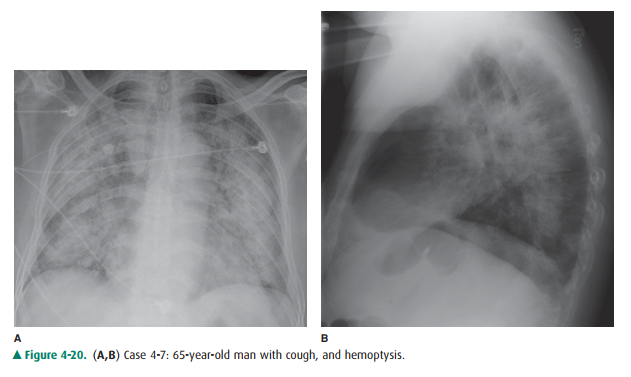
A. Diffuse airspace disease
B. Lobar airspace disease
C. Interstitial pattern
D. Unilateral airspace disease
4-8. For Figure 4-21, which one of the following best ex-plains the opacity in the right hemithorax?
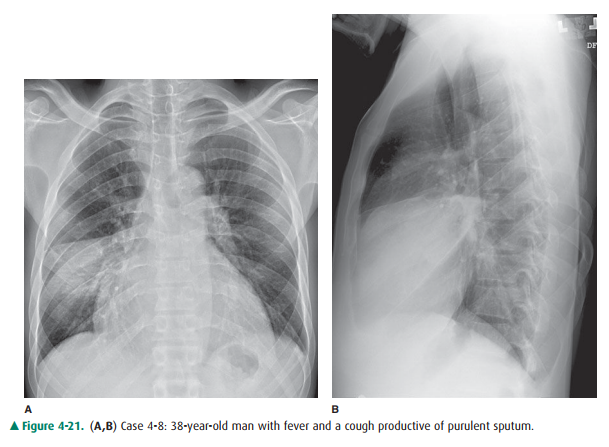
A. Collapse of the right upper lobe due to bronchial obstruction
B. Airspace consolidation of the right middle lobe
C. Empyema loculated within the right major fissure
D. Carcinoma in the right upper lobe
Radiologic Findings
(Both of these patients have airspace opacities)
4-7. In this case (Figure 4-20), the opacity involves mul-tiple lobes bilaterally (A is the correct answer to Question 4-7.).
4-8. In this case (Figure 4-21), the opacity is in the right middle lobe and obscures the medial margin of the heart. On the lateral view of this patient, the margins are sharply demarcated by the fissures, indicating thelobar nature of the process. Radiolucent structures that exhibit a branching pattern are noted to arborize through both opacities (B is the correct answer to Question 4-8.).
Discussion
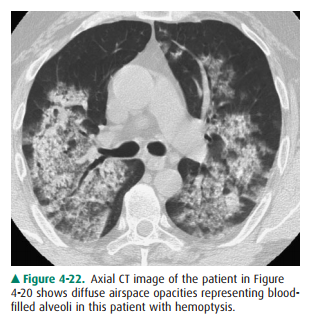
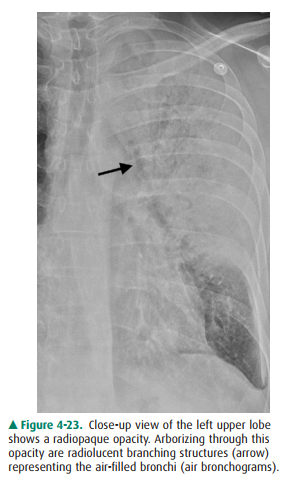
The patient in Figure 4-20 has pulmonary hemorrhage as a consequence of underlying Wegener’s granulomatosis, mani-fested as multilobar airspace disease bilaterally, also seen on CT (Figure 4-22). The patient in Figure 4-21 has pneumo-coccal pneumonia (Streptococcus pneumoniae) in the right middle lobe. The opacity seen on both radiographs is best de-scribed as airspace disease. The alveoli, or airspaces, that are normally filled with air have become filled with exudate. The exudate-filled alveoli surround the bronchi, so that the air-filled bronchi are visible as radiolucent branching structures within the more radiopaque background (Figure 4-23). Air-space disease is often lobar (Figure 4-21), multilobar, or dif-fuse (Figure 4-20) in distribution. The process may initially appear as multiple ill-defined nodules that rapidly coalesce. These nodules are the shadows of fluid-filled acini. They are 6 to 10 mm in diameter and always have ill-defined margins. The margins of these coalescing opacities are difficult to out-line. Although there can be associated volume loss as the sur-factant within the alveoli is lost, the signs of volume loss areoften subtle and do not account for the opacity seen within the lung. Once airspace disease is identified, an attempt should be made to determine its cause. Airspace disease that appears suddenly or exhibits change over hours to days is due either to pulmonary hemorrhage or to contusion, pneumo-nia, or pulmonary edema (blood, pus, or water). The pa-tient’s clinical history, physical examination, and laboratory data help to determine the most likely diagnosis. In patients likely to have infectious disorders, the responsible organism is usually not identified at first treatment, and the patient is just given antibiotics. In patients who do not respond to this initial treatment, an attempt should be made to iden-tify the organism.
In a patient with fever and productive cough, pneumonia is likely. On the other hand, a patient with rib or sternal frac-tures as a result of blunt chest trauma is more likely to have pulmonary contusion. Pulmonary edema, which may occur as a result of either cardiogenic or noncardiogenic disease.
A reticular pattern is one in which the opacities are linear in nature and the lines range from quite thin to several millime-ters thick. The opacities are oriented in multiple directions and appear to overlap so as to create the appearance of a net. This pattern is not present.
Related Topics