Chapter: Basic Radiology : Radiology of the Chest
Exercise: Interstitial Lung Disease
EXERCISE 4-15.
INTERSTITIAL LUNG DISEASE
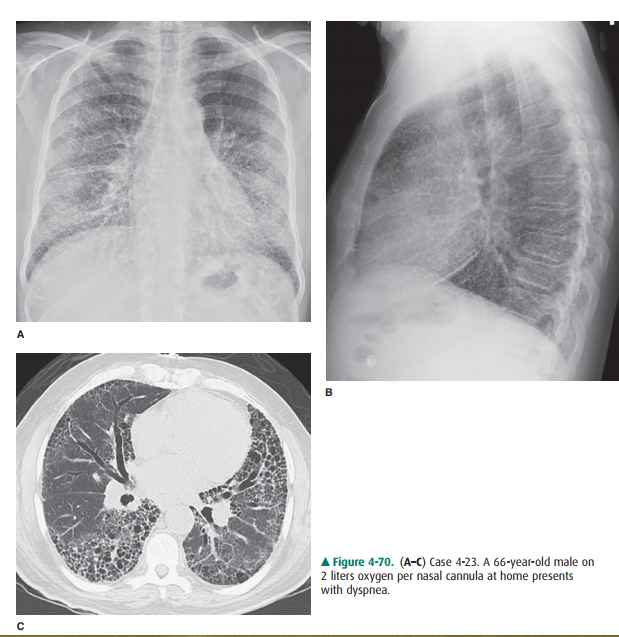
4-23. The most likely
cause for this patient’s dyspnea and pleuritic chest pain (Figure 4-70 A–C) is
A.
emphysema.
B.
empyema.
C.
pneumonia.
D.
pulmonary fibrosis.
E.
aspiration.
Radiologic Findings
4-23. The chest x-ray
(Figure 4-70 A,B) shows diffuse bilat-eral coarse interstitial opacities with
slight basilar predominance. The hemidiaphragms are flattened on the lateral
radiograph. The CT scan (Figure 4-70 C) demonstrates multiple small
similar-sized cysts stacked along the lung periphery with some preserva-tion of
normal lung centrally, particularly on the right. There is traction
bronchiectasis present as well (D is the correct answer to Question 4-23).
Discussion
The list of interstitial lung
diseases is long, and the differenti-ation can be complex. However, pulmonary
fibrosis can be readily identified. Fibrosis can be subtle, with visible linear
markings in the lung periphery on CT, or as obvious as the cystic change seen
in this patient. End-stage pulmonary fi-brosis is most readily recognized as
stacks of air-filledlucencies in the lung periphery in a pattern called
“honey-combing” (Figure 4-70 C). This is often seen as the end stage of
multiple interstitial lung diseases, most frequently in usual interstitial
pneumonitis (UIP). These patients are almost cer-tainly symptomatic, many
requiring supplemental oxygen.
Lucencies in the lung can result
from many causes. A lu-cency with a discernible wall is called a cavity. As
described in previous exercises, infectious or neoplastic etiology can result
in a cavity or air-filled lucency within the lung. However, these are rarely
small and stacked as in this case. Empyema, or an infected pleural fluid
collection, can also result in a cavity of air seen on chest radiograph. This
cavity is generally larger and unilateral. Therefore, A, B, and E are
incorrect.
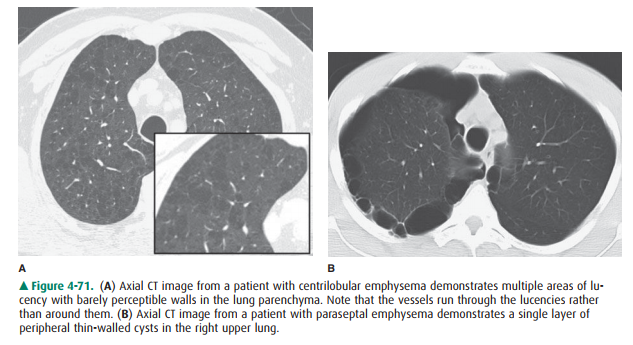
In emphysema, the air-filled
lucencies lack a discernable wall. (Figure 4-71 A). These lucencies are called
bullae and, in centrilobular emphysema, have an upper lobe preponderance.
These lucencies are not cysts,
because a true lung cyst is lined with epithelium. Emphysema is a common cause
of dyspnea and is most often smoking-related. In these patients, the lung
volumes are often larger than normal, and the lungs appear more radiolucent.
The bullous lesions of centrilobular em-physema are more easily recognized on
CT than on chest ra-diographs. Unlike other cystic lung diseases, a vessel can
generally be seen coursing through the bulla rather than around the lucency.
Another form of emphysema is parasep-tal emphysema, in which the bullae occur
along the lung pe-riphery (Figure 4-71 B).
Related Topics