Chapter: Basic Radiology : Radiology of the Chest
Exercise: Solitary Pulmonary Nodule
EXERCISE 4-6.
SOLITARY PULMONARY NODULE
4-11. Characteristics
suggesting that a nodule is benign are thatA the size
of the nodule
does not change
over 2 months.it contains central calcification. CT attenuation values
within the nodule are over 30 Hounsfield units.it is semisolid on CT.
Radiologic Findings
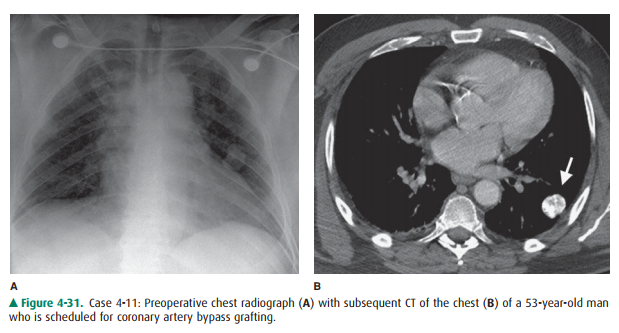
4-11. Frontal chest
radiograph (Figure 4-31 A) shows a nodule in the left mid-lung that appears
solid but is slightly lobulated. CT (Figure 4-31 B) of the chest demonstrates a
popcorn pattern of calcification (arrow) (B is the correct answer to Question
4-11).
Discussion
In attempting to determine
whether or not a nodule is be-nign, the characteristics to consider are the age
of the pa-tient, any history of previous malignancy, and the nodule’s growth
rate, density, shape, and edge characteristics. The most important of these are
the growth rate and density. If a solid nodule has had no growth over a 2-year
period and has calcification of the types associated with benign causes, then
the nodule is almost certainly benign. Because of the importance of time in
assessing growth, comparison with old images is the most important test and the
least expen-sive method of determining whether a nodule is benign. Doubling
times of lung cancers are variable, but an increase in diameter of the tumor
would be expected in a 2-year pe-riod. The absence of growth of a solid nodule
over a 2-year period is evidence that the nodule is stable is size and must,
therefore, be benign. If radiographs demonstrate growth over this 2-year
interval, then the nodule should be as-sumed to be malignant.
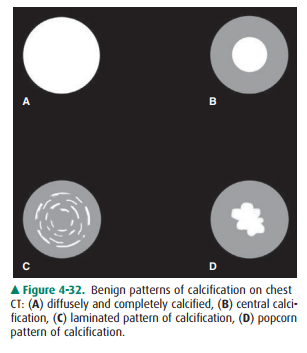
If a solid nodule is diffusely
and completely calcified (Figure 4-32 A), if it is calcified centrally (Figure
4-32 B), or if it has a laminated pattern (Figure 4-32 C), then the nod-ule may
be assumed to be benign. A popcorn pattern of cal-cification, also benign
(Figures 4-31 B, 4-32 D), can be seen in a hamartoma. Calcification may not be
apparent on the initial radiograph because the most commonly used tech-nique
for chest radiography obscures subtle calcification. Demonstration of
calcification may require fluoroscopy or repeated chest radiography with a
lower kVp technique to enhance its depiction. When it is not clear from these
studies whether calcification is present, CT should be used to iden-tify it. CT
has an extended range of tissue discrimination compared to conventional
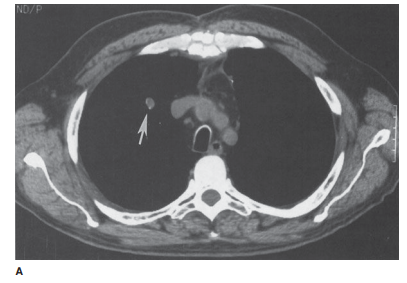
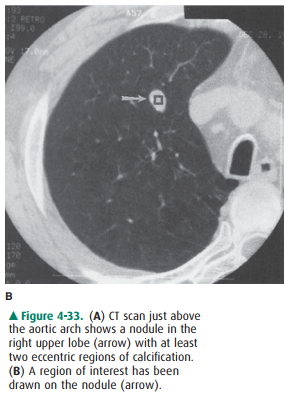
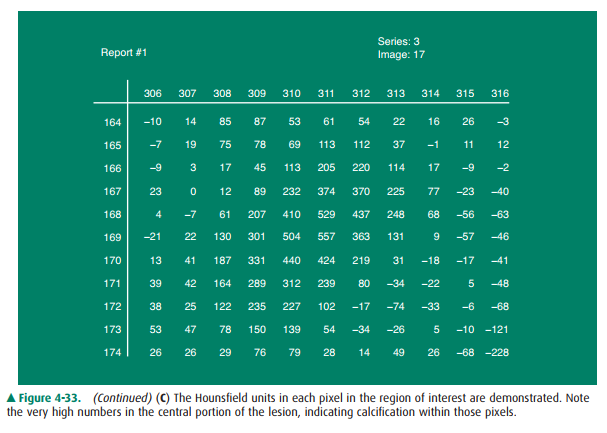
radiographs. The presence of calcification within a pulmonary nodule can be
determined by evaluating the attenuation values within a region of in-terest
(ROI) centered over the nodule (Figure 4-33 A–C). Air within the lung measures
–800 Hounsfield units, non-calcified nodules measure 30 to 100 HU, and calcified
nod-ules measure over 200 HU. Nodules with attenuation values between 0 and 200
are not necessarily malignant; they just do not have enough calcification to be
categorized unequiv-ocally as benign.If a nodule is not calcified or if it has
shown growth over 2-year period, it should be considered as a possible
malig-nancy, and further assessment should be dictated by the clin-ical
circumstances. Most patients will need evaluation for possible tissue biopsy
and surgical resection to determine the cause.
Nodules that are larger than 1 cm
in diameter are gener-ally evaluated with PET-CT. Smaller nodules are generally
considered below the threshold of resolution for this tech-nique. Nodules
considered hypermetabolic on PET-CT (in-creased radiotracer uptake relative to
background) are considered potentially malignant. Generally, these nodules then
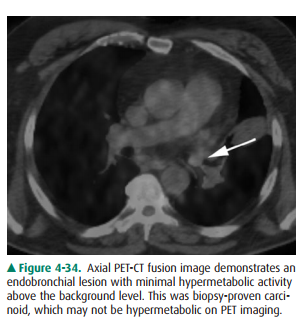
undergo percutaneous or surgical biopsy. However, whereas most cancers are hypermetabolic,
bronchoalveolar cell carcinoma (BAC) and carcinoid may not be hypermeta-bolic
(Figure 4-34). If these cancers are suspected on CT, a negative PET-CT
examination could be a false-negative and should not preclude biopsy.
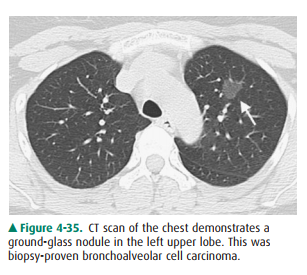
Nodules can also be ground glass
in appearance (Figure 4-35). However, this appearance is nonspecific and can be
seen in multiple etiologies including infection as well as bronchoalveolar cell
carcinoma. BAC can present as a ground-glass nodule that may not demonstrate
any signifi-cant growth over a 2-year period. Therefore, ground-glass nodules
require more extended monitoring than solid nod-ules do.
Note that the margins of the lesion, whether
smooth or spiculated, are of no value in determining the benignity or malignant
potential of a lesion. Only uniform or central calcification, absence of growth
over a 2-year period, or CT attenuation values over 200 HU throughout the
nodule are reliable noninvasive indicators of benignity.
Related Topics