Chapter: Medicine Study Notes : Gastro-Intestinal
Crohn’s Disease
Crohn’s Disease
·
= Chronic granulomatous
inflammation of the gut
Epidemiology
·
Incidence increasing. Peaks in 2nd to 3rd decade
·
1 per 1000 in UK
·
F > M, W > B
Symptoms & Signs:
·
Malaise, weight loss (65 – 75%),
failure to thrive, malabsorption
·
Diarrhoea (70 – 90%)
·
Rectal bleeding (45%)
·
Pain (50%, from inflammation,
infection, obstruction, colicky from intermittent obstruction of terminal
ileum)
·
Perianal disease (50 – 80%)
·
Mild fever (30 – 40%)
·
Anaemia, glossitis (due to
malabsorption)
·
Aphthous ulcers in mouth
·
Erythema nodosum (painful red
nodular lesions on shins), pyoderma gangrenosum (recurring skin ulcers – 10 cm),
clubbing
·
Asymptomatic periods for
weeks-months
·
Attacks may be precipitated by
emotional/physical stress
·
Risk factors: genetic, smoking,
high sugar/low fibre
Aetiology
·
Type 4 immune reaction: trigger
unknown. Cause: ?immune hyper-reactivity
·
Proposed agents: viruses,
disordered immunologic response to ingested antigen
· Genetic susceptibility. 10-fold risk in first-degree relatives
·
Þ Multifactorial ® abnormal regulation of inflammatory mediators
Investigations
·
Bloods: check for anaemia
(including anaemia of chronic disease), malabsorption, inflammatory
measurements, ESR and acute phase proteins
·
Deficiencies: folate, iron, B12,
etc, electrolyte abnormalities
·
Culture to exclude infective
causes
·
Sigmoidoscopy/colonoscopy +
biopsy
·
Upper GI endoscopy
·
Barium contrast of small &
large bowel: strictures, fistula, cobblestone appearance, skip lesions etc
Differential
·
Ileal disease: Tb, Lymphoma
·
Colonic disease: colitis
(ulcerative, ischaemic, radiation, collagenous), infection (salmonella,
shigella, campylobacter), cancer
·
Malabsorption: lactose
intolerance, coeliac disease
Pathology
·
Location:
o 75% terminal ileum
o 50% also involves colon
o 25% colon only (predominantly right side)
o <5% oesophagus, mouth
·
Macroscopic appearance:
o Skip lesions
o Transmural inflammation
o Thickened, inflexible (resembles rubber hose) with narrow lumen
o Thickened, fibrosed mesentery and enlarged regional lymph nodes
o Strictures, fistulas, abscesses
o Mucosa: varying degrees of erythema and oedema. Cobblestone mucosa
·
Microscopic appearance:
o Submucosal and subserosal inflammation with only secondary mucosal
involvement (ie glands may be straight, unaffected)
o Aphthoid ulceration of the mucosa
o Lymphocytic infiltrate, fibrosis
o Multifocal granulomatous vasculitis
o Non-caseating granulomata (only 60%): can have some Langhans/giant cells
(horseshoe pattern of nuclei around periphery of a giant cell), but usually
granulomas poorly circumscribed
Treatment
· Aim: suppress activity, restore quality of live, prevent complications
· Diet: nutritional supplements. Malnutrition a real risk, ® growth retardation in kids. May need enteral or TPN feeding for „Bowel Rest‟ ® ¯antigen load (controversial)
·
Corticosteriods e.g. prednisone:
symptomatic relief
· 5-aminosalicylic acids e.g. mezalazine
·
Antibiotics (mainly colonic and
perianal disease, ¯antigen load): metronidazole
· Steroid sparing immunosuppressives: azathioprine
· Cholestyramine: absorbs bile (normally absorbed in the terminal ileum) to stop it getting into the large bowel, where it causes irritation
·
Surgery
·
Monitor: inflammatory markers
Complications
·
Episcleritis (reddened sclera)
·
Stricture, obstruction, fistulas
(to bowel, bladder, vagina)
·
Malnutrition
·
Large & small bowel cancer
(5% at 10 years – ie small risk – not screened for)
·
Ankylosing Spondylitis
·
Pyoderma gangrenosum
·
Iritis
·
Arthritis
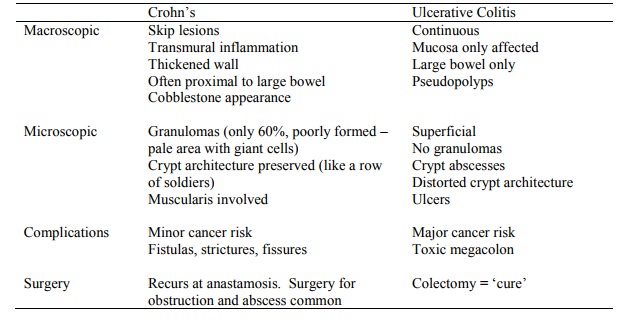
Comparison with Ulcerative Colitis
Related Topics