Chapter: Psychology: Learning
Classical Conditioning: The Relationship between the CR and the UR
The
Relationship between the CR and the UR
In Pavlov’s original studies,
dogs salivated both when they heard the CS and when they experienced the US. We
might conclude from this that the conditioned response (CR) and unconditioned
response (UR) are essentially the same behavior—and simply triggered by
different inputs. In truth, though, the CR and UR are rarely identical and are
sometimes quite different from each other.
Consider, for example, a rat that
has been conditioned to associate a flashing light with electric shock. When
the shock is actually presented, the animal jumps and squeals, and its heart
beats faster; this is the UR, triggered by the shock itself (the US). When the
animal sees the flashing light, though, its response (the CR) is different. The
animal freezes and tenses its muscles, and its heartbeat slows. This is not an
escape-from-shock reaction; instead, it’s a display of fearful anticipation.
From a biological perspective,
this result makes sense. A flashing light causes no phys-ical damage, and so
there’s no need to spend energy escaping from the light. Likewise, an animal
can’t eat a tone that has been paired with food, so there’s no point in opening
its mouth and chewing in response to the tone. In these and many other cases,
it’s sensible for the animal to react somewhat differently to the CS than it
does to the US.
So, what is the relationship
between the conditioned response (CR) and the uncondi-tioned response (UR)?
We’ve already seen that animals interpret the CS as a signal indicat-ing that
the US is about to arrive. Plausibly, then, we can think of the CS as telling
the animal to “Get ready!”—and, from this perspective, the CR is just the set
of adjustments the animal makes in preparation
for the US. If the sound of a bell has been reliably followed by food, then the
sound now signals that the animal should moisten its mouth so it will be ready
to eat when the food arrives. If the sight of a light has been followed by a
shock, then the light is a signal that the animal should stop moving around and
stay at “full alert” so it will be ready to jump as soon as the shock begins
(Domjan, 2005; P. Holland, 1984; Hollis, 1984).
Does this preparation help the
animal? It surely does. Evidence suggests, for example, that sexual activity is
more likely to lead to offspring if a CS announced the imminent arrival of the
US (the sight of a sexually receptive partner). Presumably, this is because the
CS allowed the animal to prepare itself for mating (Domjan, 2005). Likewise,
digestion is more efficient if a CS announced the imminent arrival of the US
(food in the mouth); again, the CS allowed the animal to prepare to ingest and
digest the food (Domjan, 2005; Woods & Ramsay, 2000).
CONDITIONING AND COMPENSATORY RESPONSES
Preparation for a US can take
many forms. As a remarkable illustration, consider the sit-uation of a heroin
addict. The heroin itself is a potent stimulus with many biological effects: It
decreases pain sensitivity and lifts the user’s mood. It also causes other
changes throughout the body, including drying out the mouth and various mucous
membranes.
The first few times someone uses
heroin, all of these effects are strong. If drug use continues, though, these
effects diminish. This phenomenon, which we described, is called drug
tolerance—a decrease in the response to a drug, usually result-ing from
continued use. If the person wants to keep getting the same impact from the
drug, they’ll need a larger and larger dose to offset the effect of the
tolerance.
Continued use of heroin also
leads to drug dependence and drug cravings—an inabil-ity to function
without the drug and an overwhelming desire for yet another dose, yet another
injection. The cravings are accompanied by their own set of effects—including
an increased sensitivity to pain, a
depression in the person’s mood, and an overproduc-tion of fluid in the
person’s mouth and mucous membranes.
What’s going on here? What
produces drug tolerance and drug craving? Why does the craving take the form
that it does? Answers to these questions turn out to include a key role for
classical conditioning. To understand how this works, however, we need to begin
with a point we’ll discuss more fully later where we consider the importance of
homeostasis. This term refers to the
remarkably stable environment that exists inside ofour bodies—a body
temperature that’s kept at an almost constant level, a nearly constant pH in
the bloodstream, a consistent level of glucose and oxygen in the blood, and so
on.
A drug such as heroin changes the
body’s status in many ways. In other words, heroin disrupts homeostasis; and
so, when this drug is present in the body, a range of mechanisms come into
play, all seeking to restore homeostatic stability. These mecha-nisms involve
many cellular and biochemical changes throughout the body—all designed to
repair the “disruption” caused by the drug.
But, of course, preventing a problem is always
preferable to solving the problem after it arises; avoiding disruption is better than repairing the disruption once
it’s in place. Rather than waiting until heroin disrupts the body’s state and
then responding to this disruption, it would be better if the body had a way of
dealing with the heroin disrup-tion as it
happens, so that homeostasis is never lost in the first place. This is
where clas-sical conditioning enters the scene: Thanks to conditioning, the
body begins a series of adjustments to offset the heroin’s effects even before
the drug arrives.
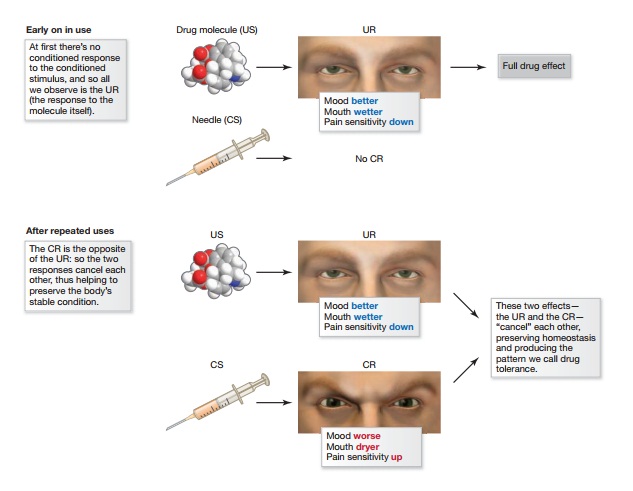
Let’s put this in concrete terms.
For a heroin user, the US is the drug itself; the UR is the body’s natural
response to the drug (Figure 7.15). The CS is complex and includes all the
stimuli that signal the drug is about to arrive—the sight of the needle,
thoughts about the drug, possibly the sights and smells of the physical
environment in which the drug is injected, and so on. But what is the CR? Here
as always, the CR will be a response that prepares the organism for the US, and
so we need to ask: What is the right preparation for heroin? If the goal is
homeostasis, then the CR should include a depression of mood in order to cancel
out heroin’s positive effects on mood; it should also include an increase in
pain sensitivity to cancel out heroin’s analgesic effects; it should include an
increase in moisture in the mucous membranes to offset heroin’s tendency to dry
out these membranes. In point after point, the CR should simply be the opposite
of the UR, so that the two will cancel each other out, leaving no overall
effect—and thus preserving homeostasis. A CR like this is referred to as a compensatory response—one that
“compensates” for the effects of the upcoming US.
Of course, when someone is
exposed to heroin for the first time, there hasn’t yet been an opportunity for
learning. Therefore, the US (the heroin) will produce the UR
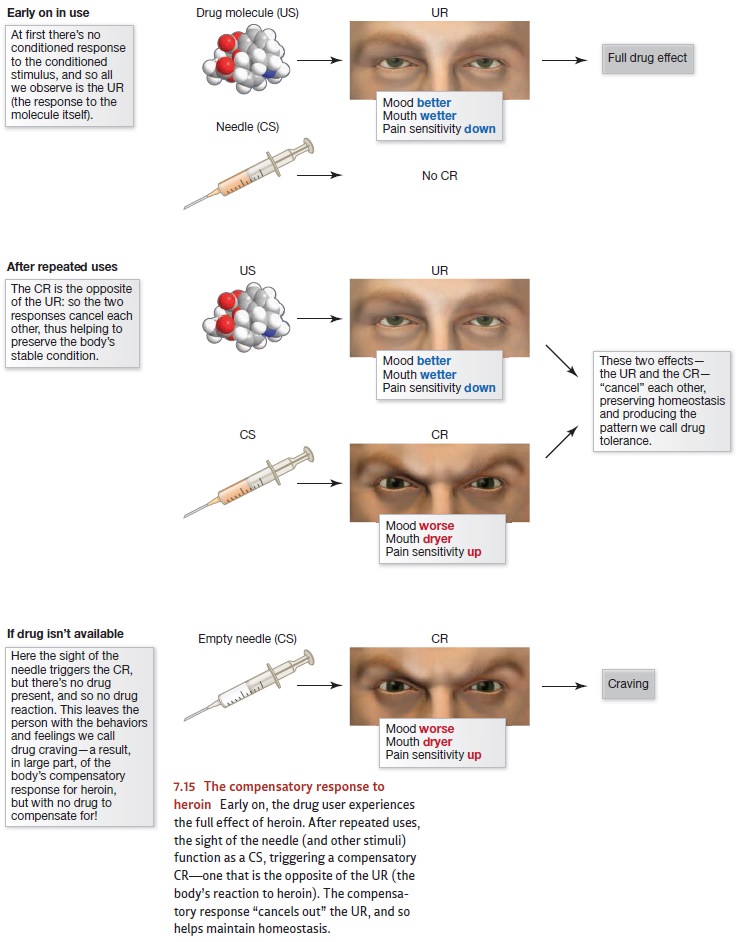
(the biological reaction to the
drug); but there will be no CR (because no learning has taken place yet). As a
result, the person will experience the drug’s full effects, and no compensatory
response will be in place (Figure 7.15, top panel). After repeated expo-sures
to the drug, though, learning will have taken place. At this point the US still
pro-duces the UR; but now, in addition, the CS elicits the compensatory CR.
This learned response, we’ve proposed, functions to “cancel out” the heroin
effects and preserve homeostasis. As a result, the UR will be less
evident—resulting in the diminished drug response that we call drug tolerance
(Figure 7.15, middle panel).
What happens if an addict sees an
empty hypodermic needle, or visits the place where he ordinarily buys or
injects the drug, but no heroin is available (Figure 7.15, bottom panel)? In
these cases the drug-associated signals all indicate that the drug will arrive
soon, but then it never arrives—so there’s a CS (the signals), but no US (no
heroin). With the CS present, the CR will be produced; but with no US, there
will be no UR. As a result, the person will experience the CR on its own—and
the CR, we’ve proposed, is the opposite of the UR. Hence the person experiences
the depression, the pain sensitivity, and so on—exactly the pattern referred to
as drug craving.
Many experiments have confirmed
these claims about heroin tolerance and craving. Among other points, the data
indicate that tolerance shows not only the pattern of gen-eralization and
discrimination that we would expect with classical conditioning but also the
familiar patterns of extinction and spontaneous recovery. In other words,
tol-erance shows the standard profile of classical conditioning, and this is
strong support for the account we’ve just sketched. Moreover, related studies
show a similar role for conditioning in tolerance observed with other drugs,
including insulin, nicotine, caf-feine, and amphetamines (Domjan, 2005; S.
Siegel, 1977, 1983; S. Siegel & Allan, 1998; S. Siegel, Kim, &
Sokolowska, 2003; Sokolowska, Siegel, & Kim, 2002). Overall, these points
provide a powerful argument that the CR is indeed best understood as a prepa-ration for the US; but it’s
important to note that this notion of preparation must beunderstood broadly.
Related Topics