Chapter: Biology of Disease: Cancer
Chemotherapy - General Treatment of Cancer
CHEMOTHERAPY
More than 100 different drugs are used to treat
different cancers. They are usually given in combination and with radiation
therapy and/or surgery. Most of the chemicals used in the treatment of cancer
are, traditionally, those that kill cells, that is they are cytotoxic. Most are
active on cells that are dividing, that is they are cycle-dependent. Drugs
which kill cells that are not dividing are noncycle-dependent. There is also
some evidence that at least some cytotoxic drugs act by inducing terminal
differentiation or apoptosis in cancer cells. Many different types of chemicals
target cell division in various ways. For example, several categories of drug
interfere with DNA synthesis. These include folic acid antagonists, alkylating
agents and purine and pyrimidine analogs and the topoisomerase inhibitors .
Other drugs inhibit cell division by disrupting the polymerization or
depolymerization of microtubules, thus interfering with the separation of
chromosomes during mitosis. Unfortunately, drugs that work by preventing cell
division do not discriminate between dividing cancer cells and dividing healthy
cells. Thus, these drugs have considerable toxicity, particularly towards bone
marrow and the epithelial cells of the skin and GIT. Thus, chemotherapy is
associated with anemia, nausea and damage to the actively dividing cells of the
hair follicles, leading to considerable, but usually reversible, hair loss. A
role of the hospital pharmacist is to advise on treatment to minimize the
discomfort caused by this therapy. In the treatment of some cancers, aggressive
chemotherapy may destroy bone marrow, such that patients require a bone marrow
transplant .
The route of administration of chemotherapeutic
agents depends on the drug. Many drugs are administered intravenously by
infusion. Others are administered intrathecally, that is, by injection into the
innermost membrane surrounding the central nervous system. This is usually
achieved by lumbar puncture. Administration of chemotherapy in hospitals
requires the hospital pharmacist to work alongside the physician so that the
most appropriate dose is administered in the most suitable manner. Some of the
drugs used to treat cancer are discussed below, although this list is by no
means exhaustive. It is worth noting that a natural selection process often
takes place within tumors treated with chemotherapy, in that some of the tumor
cells may develop resistance to the drug. In cases of drug resistance it is
necessary to change the chemotherapeutic agent.
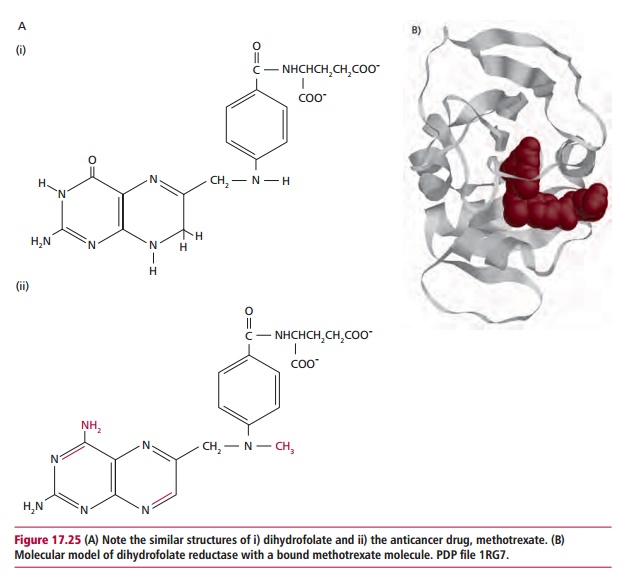
Dihydrofolate reductase (DHFR) is active in the
synthesis of tetrahydrofolate, which is required for the synthesis of purines
and pyrimidines, themselves required for the synthesis of nucleotides and DNA.
Folic acid antagonists inhibit the DHFR and some, such as methotrexate, which
is cytotoxic in concentrations between 10–7 and 10–8 mol dm–3 are used in
the treatment of cancer. Methotrexate closely resembles the substrate for
dihydrofolate reductase and can bind to it, inhibiting its action (Figure 17.25).
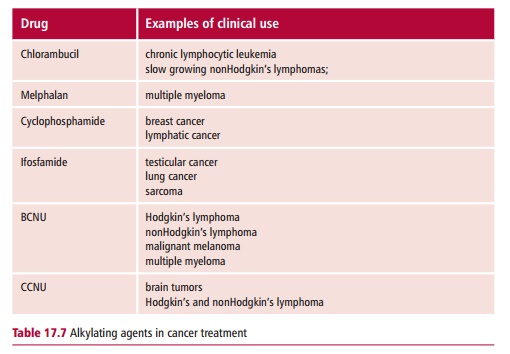
Alkylating agents that have two reactive groups are
bifunctional and can cross-link two biomolecules. Cross-linking the two strands
of DNA is the major cause of toxicity of these drugs since this prevents the
separation of the strands which is required for the synthesis of new DNA.
Examples of alkylating agents include the nitrogen mustards, such as
cyclophosphamide, melphalan, ifosfamide and chlorambucil, and the nitrosoureas,
for example bis-chloro-ethyl
nitrosourea (BCNU; carmustine) and cyclohexyl-chloroethyl nitroso-urea (CCNU;
lomustine). Some examples of their use is shown in Table 17.7.
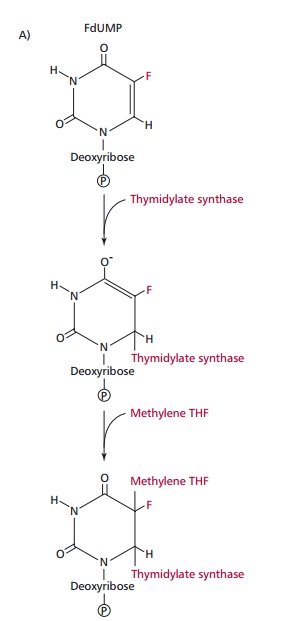
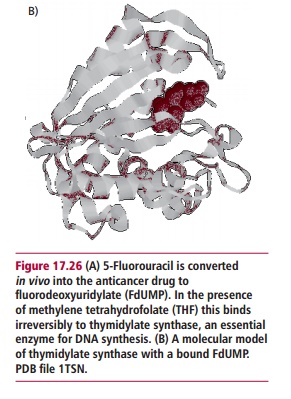
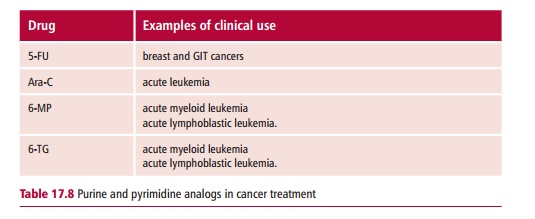
Purine and pyrimidine analogs are drugs that resemble
one of the bases found in DNA and/or RNA. When present during nucleic acid
synthesis, they interfere with the synthesis of DNA, though the site at which
they exert their effects depends on the drug itself. Pyrimidine analogs include
5-fluorouracil or 5-FU (Figure 17.26)
and cytidine arabinoside (ara-C). Purine analogs include 6-mercaptopurine
(6-MP) and 6-thioguanine. Table 17.8
lists some of their uses in cancer treatment.
Microtubules form the mitotic spindle, which is
essential for the process of chromosome separation during mitosis and meiosis.
The formation of a spindle requires microtubules to polymerize from tubulin
subunits, whereas separation of chromosomes requires depolymerization. Any drug
which interferes with either of these processes will interfere with cell
division. The first drug shown to prevent polymerization was colchicine,
originally obtained from the autumn crocus, Colchicum
officinale, though this is too toxic for
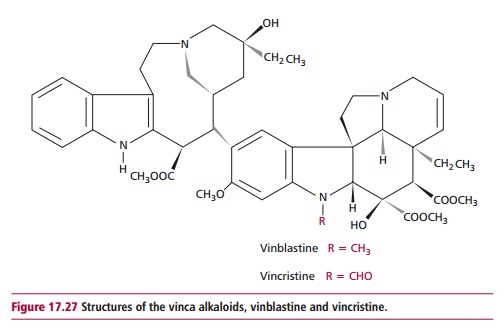
therapeutic use. The vinca alkaloids vincristine,
vinblastine and vinorelbine (Figure 17.27),
all derived originally from the periwinkle plant Vinca rosea, work in a similar manner to colchicine. Vinblastine is
used in combination with other drugs to treat testicular cancer, while
vincristine is used in treating leukemias. Vinorelbine is used in lung and
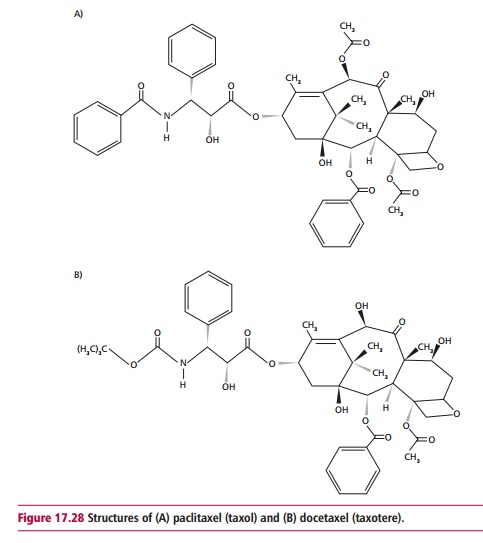
breast cancer therapy. Paclitaxel, otherwise known as taxol, and docetaxel or
Taxotere (Figure 17.28) are derived
from the bark and needles of the Pacific yew tree, Taxus brevifolia (Figure 15.8
(B)). These drugs also target microtubules but in this case they prevent
their de-polymerization. Both drugs are used in the treatment of ovarian,
breast and lung cancer.
Topoisomerase inhibitors form a complex with DNA
topoisomerase II and inhibit DNA replication. Examples of this class of drugs
include VP-16, or etoposide, and VP-26, or teniposide, both of which are
derivatives of podophyllotoxin, which is derived from the mandrake plant, Madragora. VP-16 is used in the
treatment of small cell lung cancer, testicular cancer and lymphomas and VM-26
is used to treat childhood leukemia.
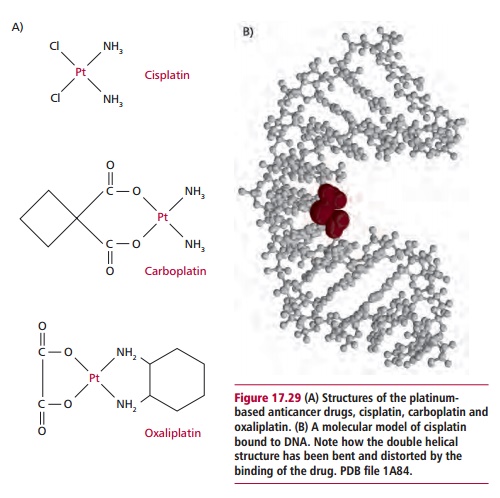
Cisplatin (cis-diamminedichloroplatinum)
was first discovered in experiments that showed that the growth of bacteria was
inhibited by an electric current delivered by platinum electrodes. This drug is
now used in combination therapy to treat testicular cancer. It is also used in
treating lung cancer. Other platinum-based drugs include carboplatin and
oxaliplatin and all function by binding to DNA, cross-linking the strands and
distorting its double helical shape (Figure
17.29 (A) and (B)). This facilitates the binding of other proteins to the
DNA molecule that mediate toxicity of the drug.
Tumor-specific molecules, on the surfaces of cancer
cells may be targeted with monoclonal antibodies . In this way treatment should
be more directed at the tumor and general toxicity reduced. Over the years,
several approaches have been made to producing targeted therapy using these antibodies.
For example, antibodies have been used to target cytotoxic drugs and toxins
such as ricin directly at tumor cells, the so-called ‘Magic bullet’ therapy.
However, since monoclonal antibodies are mouse immunoglobulin they stimulate an
immune response in humans. Hence, antibodies have been engineered to contain
mouse binding sites but which are carried on human constant regions . Examples
of monoclonal antibodies currently in use are trastuzumab (Herceptin), which is
licensed for the treatment of secondary breast cancer and which is directed at
growth factor receptors on the tumor cells, and rituximab (Rituxan) which is
used in the treatment of nonHodgkin’s lymphoma.
Related Topics