Chapter: Modern Pharmacology with Clinical Applications: Pharmacological Management of Chronic Heart Failure
Cardiac Electrophysiology: Reentry
Reentry
Reentry is an abnormality of
impulse conduction wherein an excitatory wavefront circulates around an
inexcitable region. Figures 16.5 and 16.6 show a nor-mally propagated and a
reentrant event in injured ven-tricular myocardium, respectively. As
illustrated in Figure 16.5, the wave of excitation passes through ho-mogeneous
tissue involving the Purkinje system (P1 and P2) and
enters normal ventricular myocardium. As indi-cated in the figure, the wave of
excitation conducts around an inexcitable barrier, collides within the tissue,
and extinguishes within the ventricular myocardium. A normally propagating
impulse will enter ventricular myocardium nearly simultaneously at multiple
regions where Purkinje fibers terminate in the walls of both ven-tricles. The
sequence of activation of the ventricular
myocardium is rapid (~0.04 second). The net result is orderly activation of
all ventricular myocardial fibers, giving rise to normal-appearing action
potentials in the respective regions and a normal electrocardiogram.
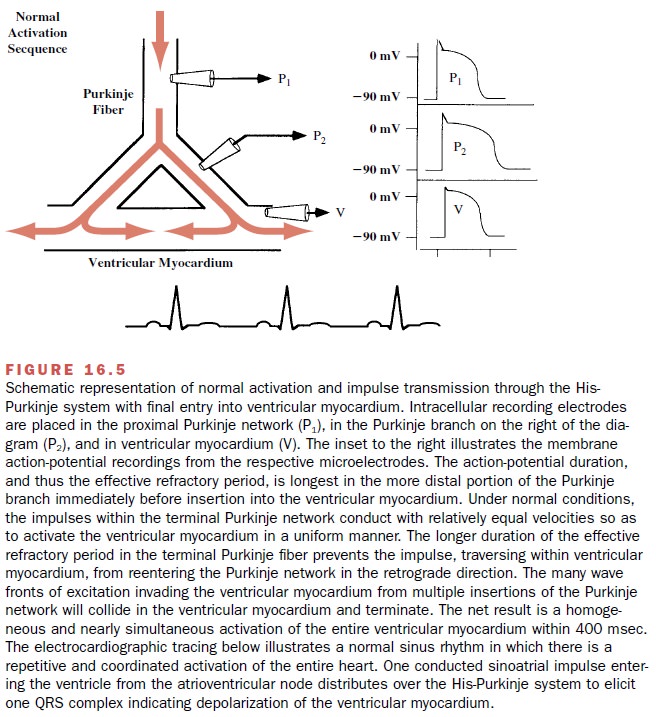
In the undamaged myocardium,
cardiac impulses travel rapidly antegrade through the Purkinje fibers to
deliver the excitatory electrical impulse to the ventricu-lar myocardium.
During the normal activation se-quence, retrograde conduction from ventricular
myo-cardium to the conducting fibers is prevented by the longer duration of the
membrane action potential and thus the refractory period in the Purkinje
fibers.
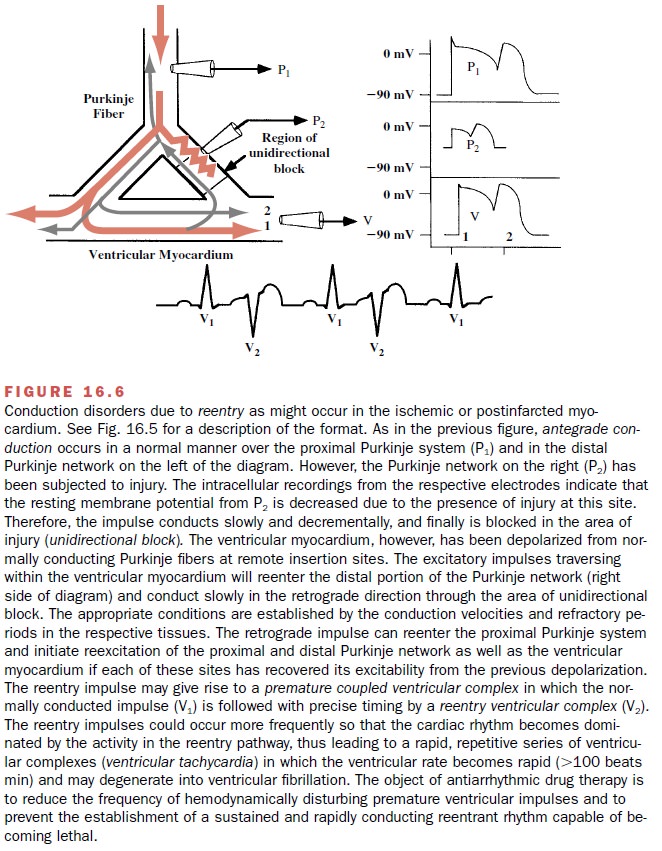
In the presence of myocardial
ischemia, propaga-tion of cardiac impulses may be interfered with and a
functional unidirectional block may occur. Impulses may fail to conduct longer
in the anterograde direction to excite the more distal ventricular myocardium.
Thus, the terminal segments of the Purkinje fibers within the affected region
may be activated by impulses passing from the ventricular myocardium to conduct
in a retro-grade direction (impulse 1, Fig. 16.6), albeit at a slower rate of
conduction. In some situations, the retrograde impulse will enter an area of
normal myocardium suffi-ciently repolarized that it is no longer refractory,
and a propagated action potential will result. The generation of an action
potential may produce an increased rate of ventricular activation and may
become self-sustaining. The latter phenomenon is known as a reentrant, or cir-cus, rhythm. If propagation is too rapid through the re-gion of
myocardial damage, the retrograde impulse will attempt to reenter the normal
region while the tissue is refractory. This will give rise to bidirectional
block, ter-minating the reentrant wave front. Therefore, for reen-try to occur, there must be a
region of unidirectional block and slow conduction. The delay in
conduction permits the tissue ahead
of the advancing wave front to regain its excitability, sustaining the reentry
circuit. As shown in Figure 16.6, the reentrant wave front gives rise to a
second depolarizing impulse (2) in the ventric-ular myocardium and in each of
the branches of the Purkinje network (P1 and P2). The net
result of the reentrant wave is depicted in the electrocardiogram (ECG), in
which coupled ventricular premature com-plexes (V2) follow each
normal (V1) complex.
It is estimated that 80 to 90% of clinical arrhythmias have a
reentry mechanism. One explanation of how an antiarrhythmic
agent may abolish reentry is by convert-ing unidirectional block to
bidirectional block. A sec-ond mechanism to explain the action of
antiarrhythmic drugs is that they can prevent reentry by increasing the ERP of
the cardiac fibers within or surrounding the re-gion of the reentrant circuit.
Related Topics