Chapter: Essentials of Anatomy and Physiology: Respiratory System
Ventilation and Respiratory Volumes
VENTILATION AND RESPIRATORY VOLUMES
Ventilation, orbreathing,is the process of moving air into and outof the lungs. There are two phases of ventilation: (1) Inspiration, or inhalation, is the movement of air into the lungs; (2)expiration,orexhalation, is the movement of air out of the lungs. Ventilation isregulated by changes in thoracic volume, which produce changes in air pressure within the lungs.
Changing thoracic Volume
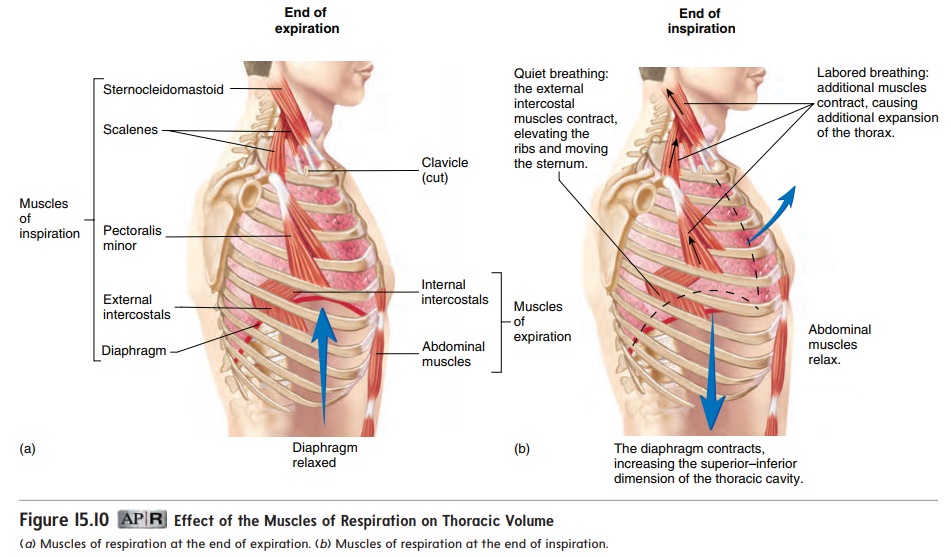
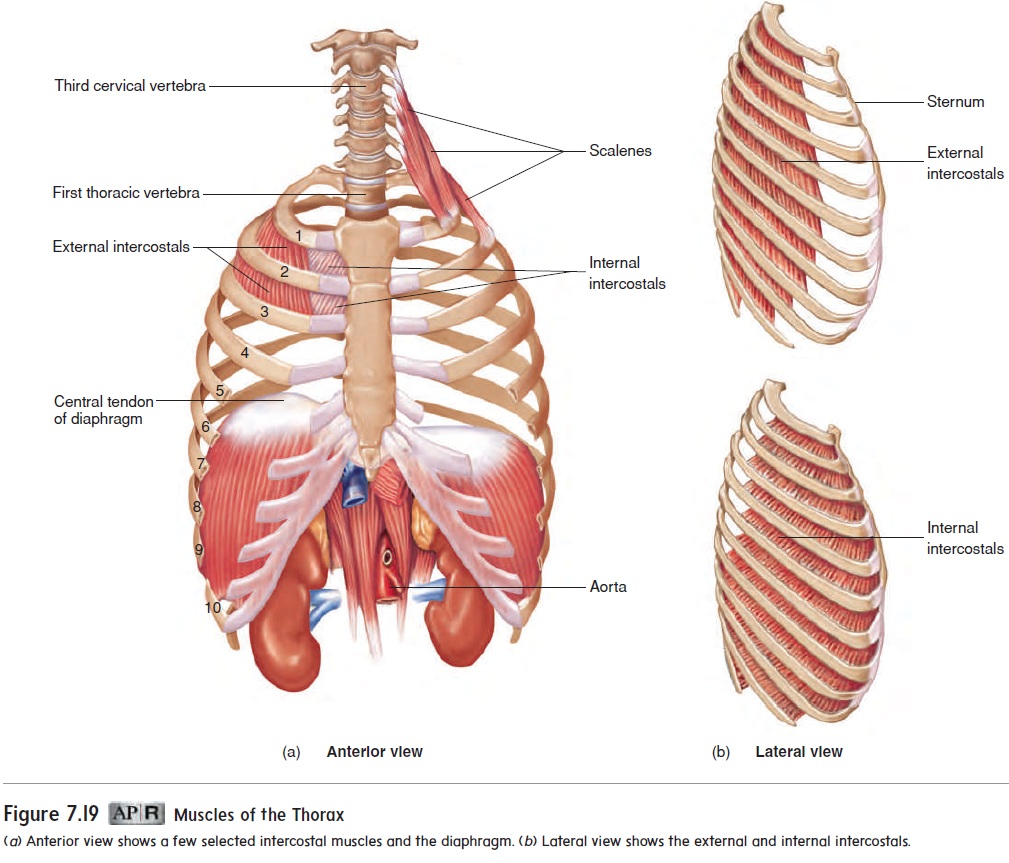
The muscles associated with the ribs are responsible for ventila-tion (figure 15.10). The muscles of inspiration include the dia-phragm and the muscles that elevate the ribs and sternum, suchas the external intercostals. The diaphragm (dı̄′ a-fram; partition) is a large dome of skeletal muscle that separates the thoracic cavity from the abdominal cavity (see figure 7.19). The musclesof expiration, such as the internal intercostals, depress the ribsand sternum.
At the end of a normal, quiet expiration, the respiratory muscles are relaxed (figure 15.10a). During quiet inspiration, contraction of the diaphragm causes the top of the dome to move inferiorly, which increases the volume of the thoracic cavity. The largest change in thoracic volume results from movement of the diaphragm. Contraction of the external intercostals also elevates the ribs and sternum (figure 15.10b), which increases thoracic volume by increasing the diameter of the thoracic cage.
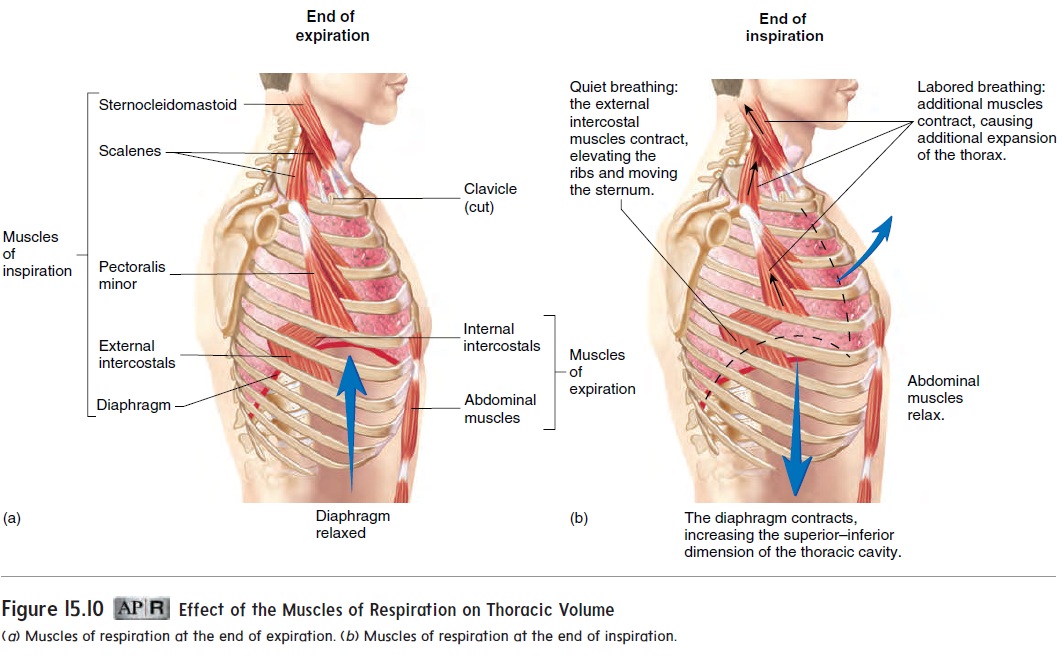
Expiration during quiet breathing occurs when the diaphragm and external intercostals relax and the elastic properties of the thorax and lungs cause a passive decrease in thoracic volume.
There are several differences between normal, quiet breathing and labored breathing. During labored breathing, all the inspira-tory muscles are active, and they contract more forcefully than during quiet breathing, causing a greater increase in thoracic volume (figure 15.10b). Also during labored breathing, forceful contraction of the internal intercostals and the abdominal muscles produces a faster and greater decrease in thoracic volume than would be produced by the passive recoil of the thorax and lungs.
Pressure Changes and Airflow
A. Two physical principles govern the flow of air into and out of the lungs:
1. Changes in volume result in changes in pressure. As thevolume of a container increases, the pressure within the container decreases. The opposite is also true. As the volume of a container decreases, the pressure within the container increases. In the same way, the muscles of respiration change the volume of the thorax and therefore the pressure within the thoracic cavity.
2. Air flows from an area of higher pressure to an area of lower pressure. If the pressure is higher at one end of a tubethan at the other, air or fluid flows from the area of higher pressure toward the area of lower pressure. The greater the pressure difference, the greater the rate of airflow. Air flows through the respiratory passages because of pressure differences between the outside of the body and the alveoli inside the body. These pressure differences are produced by changes in thoracic volume.
The volume and pressure changes responsible for one cycle of inspiration and expiration can be described as follows:
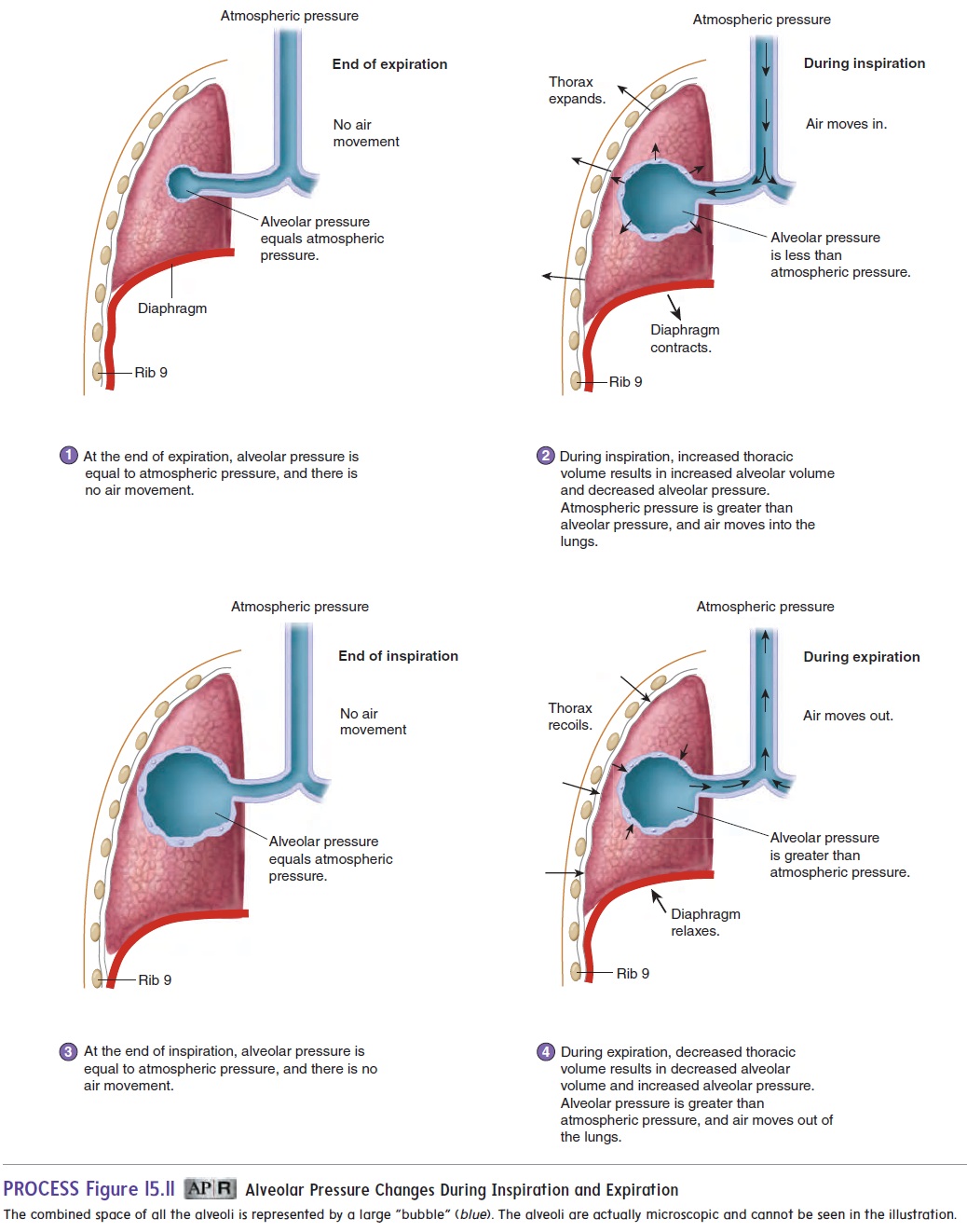
1. At the end of expiration, alveolar pressure, which is the air pressure within the alveoli, is equal to atmosphericpressure, which is the air pressure outside the body. No airmoves into or out of the lungs because alveolar pressure and atmospheric pressure are equal (figure 15.11, step 1).
2. During inspiration, contraction of the muscles of inspiration increases the volume of the thoracic cavity. The increased thoracic volume causes the lungs to expand, resulting in an increase in alveolar volume (see “Changing Alveolar Volume” later in this section). As the alveolar volume increases, alveolar pressure becomes less than atmospheric pressure, and air flows from outside the body through the respiratory passages to the alveoli (figure 15.11, step 2).
3. At the end of inspiration, the thorax and alveoli stop expanding. When the alveolar pressure and atmospheric pressure become equal, airflow stops (figure 15.11, step 3).
4. During expiration, the thoracic volume decreases, producing a corresponding decrease in alveolar volume. Consequently, alveolar pressure increases above atmospheric pressure, and air flows from the alveoli through the respiratory passages to the outside (figure 15.11, step 4).
As expiration ends, the decrease in thoracic volume stops, and the process repeats, beginning at step 1.
Lung Recoil
During quiet expiration, thoracic volume and lung volume decrease because of lung recoil, the tendency for an expanded lung to decrease in size. The thoracic wall also recoils due to the elastic properties of its tissues. Lung recoil is able to occur because the connective tissue of the lungs contains elastic fibers and because the film of fluid lining the alveoli has surface tension. Surface tension exists because the oppositely charged ends of water molecules are attracted to each other . As the water molecules pull together, they also pull on the alveolar walls, causing the alveoli to recoil and become smaller.
Two factors keep the lungs from collapsing: (1) surfactant and(2) pressure in the pleural cavity.
Surfactant
Surfactant (ser-fak′tănt;surfaceactingagent) is a mixture oflipoprotein molecules produced by secretory cells of the alveolar epithelium. The surfactant molecules form a single layer on the surface of the thin fluid layer lining the alveoli, reducing surface ten-sion. Without surfactant, the surface tension causing the alveoli to recoil can be ten times greater than when surfactant is present. Thus, surfactant greatly reduces the tendency of the lungs to collapse.
Pleural Pressure
When pleural pressure, the pressure in the pleural cavity, is less than alveolar pressure, the alveoli tend to expand. This principle can be understood by considering a balloon. The balloon expands when the pressure outside it is less than the pressure inside. This pressure difference is normally achieved by increasing the pressure inside the balloon by blowing into it. This pressure difference, however, can also be achieved by decreasing the pressure outside the balloon. For example, if the balloon is placed in a chamber from which air is removed, the pressure around the balloon becomes lower than atmo- spheric pressure, and the balloon expands. The lower the pressure outside the balloon, the greater the tendency for the higher pres- sure inside the balloon to cause it to expand. In a similar fashion, decreasing pleural pressure can result in expansion of the alveoli.
Normally, the alveoli are in the expanded state because pleural pressure is lower than alveolar pressure. Pleural pressure is lower than alveolar pressure because of a suction effect caused by fluid removal by the lymphatic system and by lung recoil. As the lungs recoil, the visceral and parietal pleurae tend to be pulled apart. Normally, the lungs do not pull away from the thoracic wall because pleural fluid holds the visceral and parietal pleurae together. Nonetheless, this pull decreases pressure in the pleural cavity. You can appreciate this effect by putting water on the palms of your hands and then placing them together. As you gently pull your hands apart, you will feel a sensation of negative pressure.
When pleural pressure is lower than alveolar pressure, the alveoli tend to expand. This expansion is opposed by the tendency of the lungs to recoil. Therefore, the alveoli expand when the pleural pressure is low enough that lung recoil is overcome. If the pleural pressure is not low enough to overcome lung recoil, the alveoli collapse, as is the case with a pneumothorax (see the Clinical Impact: “Pneumothorax”).
Changing Alveolar Volume
Changes in alveolar volume cause the changes in alveolar pressure that are responsible for moving air into and out of the lungs (see figure 15.11). Alveolar volume changes result from changes in pleural pressure. For example, during inspiration, pleural pressure decreases, and the alveoli expand. The decrease in pleural pressure occurs for two reasons:
1. Increasing the volume of the thoracic cavity results in a decrease in pleural pressure because a change in volume affects pressure.
2. As the lungs expand, lung recoil increases, increasing the suction effect and lowering the pleural pressure. The increased lung recoil of the stretched lung is similar to the increased force generated in a stretched rubber band.
The events of inspiration and expiration can be summarized as follows:
1. During inspiration, pleural pressure decreases because of increased thoracic volume and increased lung recoil. As pleural pressure decreases, alveolar volume increases, alveolar pressure decreases, and air flows into the lungs.
2. During expiration, pleural pressure increases because of decreased thoracic volume and decreased lung recoil. As pleural pressure increases, alveolar volume decreases, alveolar pressure increases, and air flows out of the lungs.
Respiratory Volumes and Capacities
Spirometry (sp -rom′-tr ) is the process of measuring volumesof air that move into and out of the respiratory system, and the spirometer (sp -rom′-ter) is the device that measures these respi-ratory volumes. Measurements of the respiratory volumes can provide information about the health of the lungs. Respiratoryvolumes are measures of the amount of air movement during dif-ferent portions of ventilation, whereas respiratory capacities are sums of two or more respiratory volumes. The four respiratory volumes and their normal values for a young adult male are shown in figure 15.12:
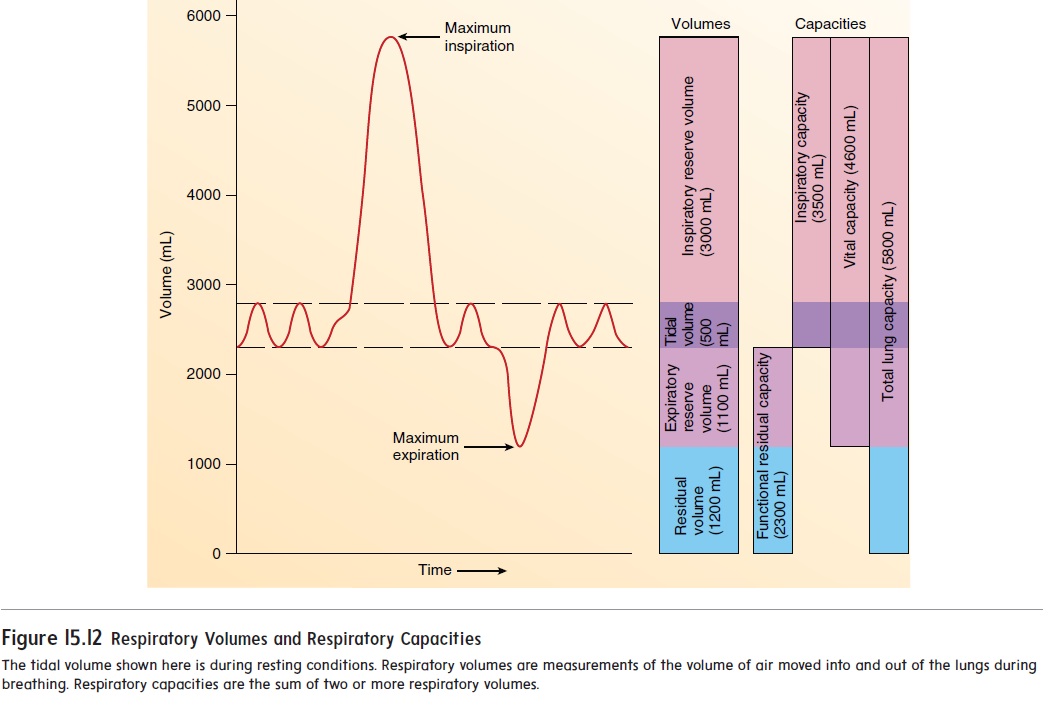
1. Tidal volume is the volume of air inspired or expired witheach breath. At rest, quiet breathing results in a tidal volume of about 500 milliliters (mL).
2. Inspiratory reserve volume is the amount of air that canbe inspired forcefully beyond the resting tidal volume (about 3000 mL).
3. Expiratory reserve volume is the amount of air that canbe expired forcefully beyond the resting tidal volume (about 1100 mL).
4. Residual volume is the volume of air still remaining in therespiratory passages and lungs after maximum expiration (about 1200 mL).
The tidal volume increases when a person is more active. Because the maximum volume of the respiratory system does not change from moment to moment, an increase in the tidal volume causes a decrease in the inspiratory and expiratory reserve volumes.
Values of respiratory capacities, the sum of two or more pul-monary volumes, are shown in figure 15.12:
1. Functional residual capacity is the expiratory reservevolume plus the residual volume. This is the amount of air remaining in the lungs at the end of a normal expiration (about 2300 mL at rest).
2. Inspiratory capacity is the tidal volume plus the inspiratoryreserve volume. This is the amount of air a person can inspire maximally after a normal expiration (about3500 mL at rest).
3. Vital capacity is the sum of the inspiratory reserve volume,the tidal volume, and the expiratory reserve volume. It is the maximum volume of air that a person can expelfrom the respiratory tract after a maximum inspiration (about 4600 mL).
4. Total lung capacity is the sum of the inspiratory andexpiratory reserves and the tidal and residual volumes (about 5800 mL). The total lung capacity is also equal to the vital capacity plus the residual volume.
Factors such as sex, age, and body size influence the respira-tory volumes and capacities. For example, the vital capacity of adult females is usually 20–25% less than that of adult males. The vital capacity reaches its maximum amount in young adults and gradually decreases in the elderly. Tall people usually have a greater vital capacity than short people, and thin people have a greater vital capacity than obese people. Well-trained athletes can have a vital capacity 30–40% above that of untrained people. In patients whose respiratory muscles are paralyzed by spinal cord injury or diseases such as poliomyelitis or muscular dystrophy, the vital capacity can be reduced to values not consistent with survival (less than 500–1000 mL).
The forced expiratory vital capacity is the rate at which lung volume changes during direct measurement of the vital capacity. It is a simple and clinically important pulmonary test. The individual inspires maximally and then exhales maximally as rapidly as possible into a spirometer. The spirometer records the volume of air expired per second. This test can help identify conditions in which the vital capacity might not be affected but the expiratory flow rate is reduced. Abnormalities that increase the resistance to airflow slow the rate at which air can be forced out of the lungs. For example, in people who have asthma, contraction of the smooth muscle in the bronchioles increases the resistance to airflow. In people who have emphysema, changes in the lung tissue result in the destruction of the alveolar walls, collapse of the bron-chioles, and decreased elasticity of the lung tissue. The collapsed bronchioles increase the resistance to airflow. In people who have chronic bronchitis, the air passages are inflamed. The swelling, increased mucus secretion, and gradual loss of cilia result in narrowed bronchioles and increased resistance to airflow.
Related Topics