Chapter: Clinical Dermatology: Regional dermatology
The nail in systemic disease
The nail
in systemic disease
The nails can provide useful clues for general physicians.
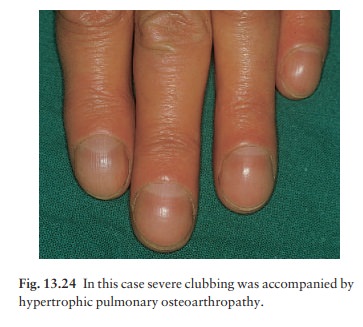
Clubbing (Fig.
13.24) is a bulbous enlargementof the terminal phalanx with an increase in the
angle between the nail plate and the proximal fold to over 180° (Fig. 13.25).
Its association with chronic lung disease and with cyanotic heart disease is
well known. Rarely clubbing may be familial with no underlying cause. The
mechanisms involved in its formation are still not known.

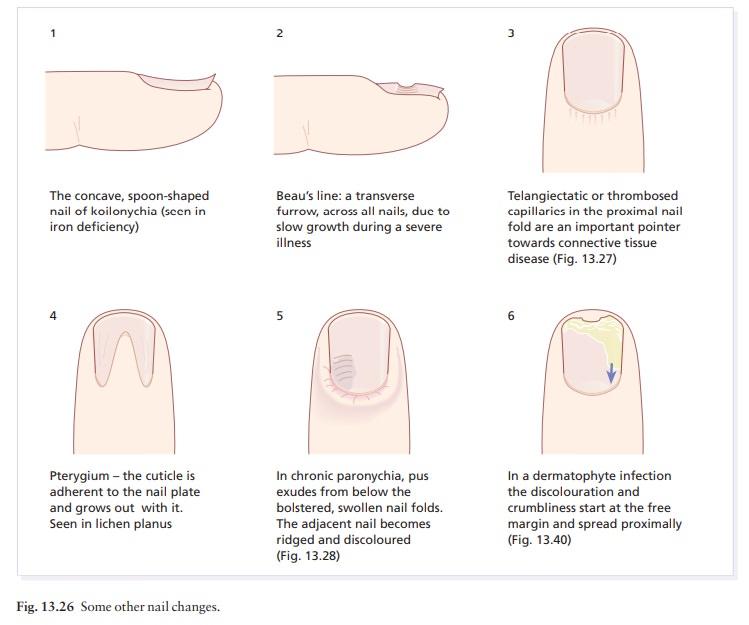
Koilonychia,
a spooning and thinning of the nailplate, indicates iron deficiency (Fig.
13.26).
Colour
changes: the ‘half-and-half’ nail, with awhite proximal and red or
brown distal half, is seen in a minority of patients with chronic renal
failure. Whitening of the nail plates may be related to hypo-albuminaemia, as
in cirrhosis of the liver. Some drugs, notably antimalarials, antibiotics and
phenothiazines, can discolour the nails.
Beau’s
lines are transverse grooves which appearsynchronously on all
nails a few weeks after an acute illness, and which grow steadily out to the
free margin (Fig. 13.26).
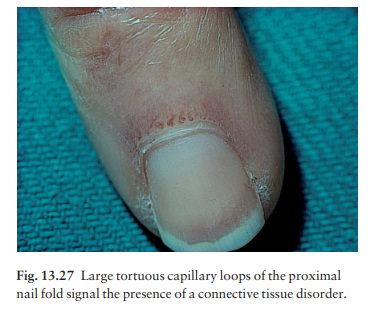
Connective
tissue disorders: nail fold telangiectasia orerythema is a useful physical
sign in dermatomyositis, systemic sclerosis and systemic lupus erythematosus
(Fig. 13.27). In dermatomyositis the cuticles become shaggy, and in systemic
sclerosis loss of finger pulp leads to overcurvature of the nail plates. Thin
nails, with longitudinal ridging and sometimes partial onycholysis, are seen
when the peripheral circulation is impaired, as in Raynaud’s phenomenon.
Related Topics