Chapter: Basic Radiology : Radiology of the Chest
Exercise: Pulmonary Neoplasm
EXERCISE 4-7. PULMONARY NEOPLASM
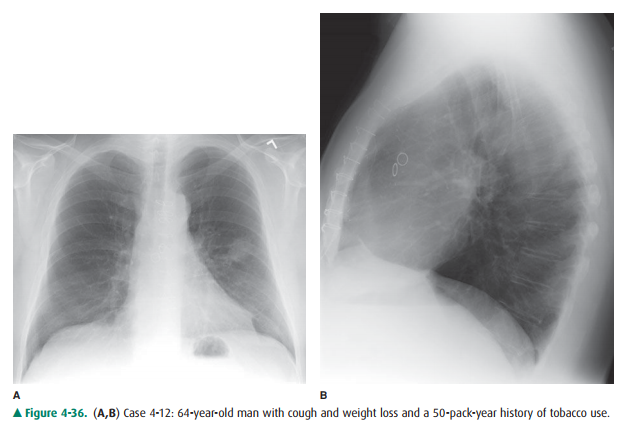
4-12. The best description of the chest radiograph in Fig-ure 4-36 A,B is
A. mass in the left upper lobe.
B. left upper lobe collapse.
C. mediastinal mass.
D. consolidation of the left upper lobe.
E. enlargement of the left pulmonary artery.
Radiologic Findings
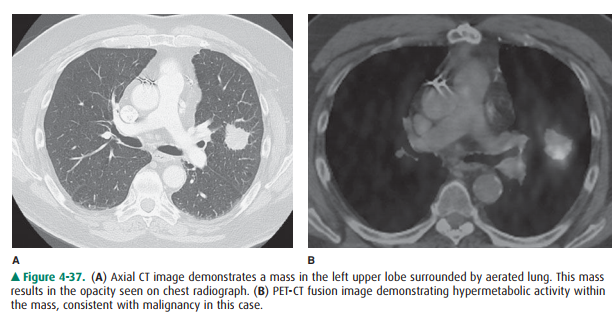
4-12. In this case, the chest radiographs show a smoothly marginated opacity projecting over the left upper lobe. Both hila are normal in size. The opacity seen on the PA view is smaller than the volume of the left upper lobe, and no air bronchograms are present; this excludes consolidation of the lung as an answer. The posterior margin of the opacity is not a long straight or gently curving line, as is the major fissure, and therefore left upper lobe atelectasis is not the cor-rect answer. The one best description of the radi-ographic findings is mass in the left upper lobe (A is the correct answer to Question 4-12). In a patient with cough, weight loss, and a history of tobacco use, bronchogenic carcinoma should be the primary con-sideration. A CT examination in this patient (Figure 4-37 A) shows the mass in the left upper lobe, com-pletely surrounded by aerated lung. PET-CT fusion imaging (Figure 4-37 B) demonstrates the expected hypermetabolic activity in the left upper lobe mass. A CT-guided percutaneous biopsy of this mass yielded a diagnosis of adenocarcinoma.
Discussion
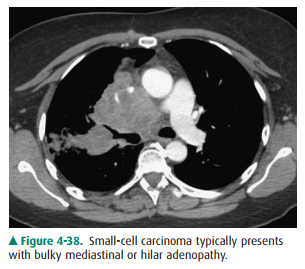
There are more than 220,000 new cases of lung cancer, or bronchogenic carcinoma, and 160,000 deaths from lung cancer in the United States each year. Bronchogenic carci-noma is the more appropriate term, as most of them arise from the epithelium of the airways and not the lung per se. Because early recognition and surgical resection offer the pa-tient the best chance for cure, it is important to be familiar with the variety of radiographic appearances of lung cancer. Four major cell types account for almost 90% of all lung can-cers. The major cell types are squamous cell, adenocarcinoma, large cell, and small cell. For therapeutic purposes, lung can-cer is divided into small-cell and non-small-cell lung cancer (NSCLC). This distinction is necessary because small-cell bronchogenic carcinoma is almost always widespread at the time of diagnosis and is best treated by chemotherapy and ra-diation therapy. Non-small-cell bronchogenic carcinoma, on the other hand, is best treated by surgical resection when the tumor is confined to one lung and regional lymph nodes. The typical radiographic appearance of small-cell carcinomais bulky hilar and/or mediastinal lymph nodes; the primary tumor sometimes is visible as a nodule within the lung (Figure 4-38).
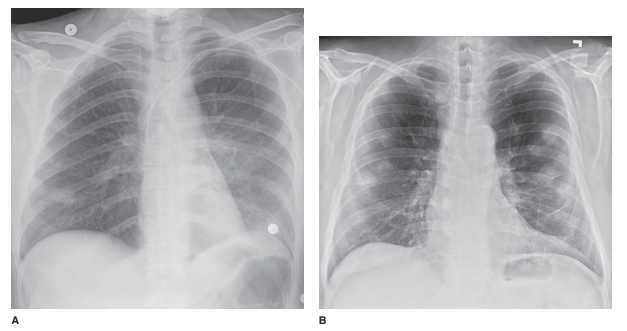
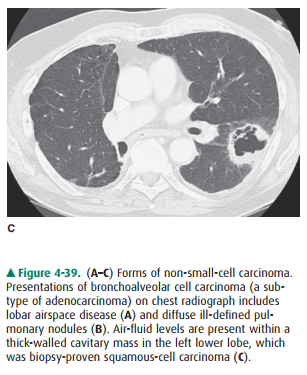
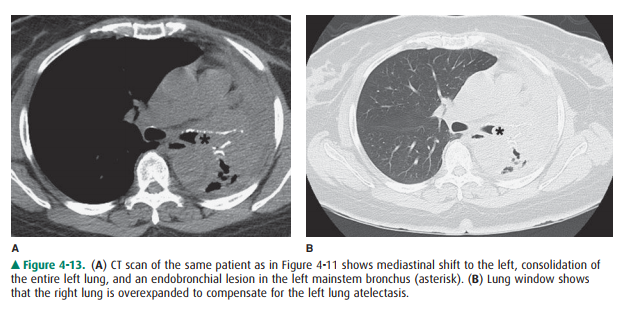
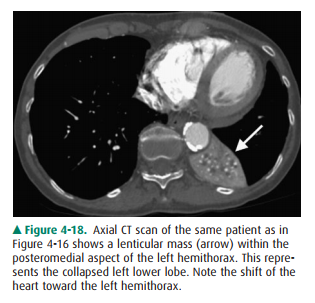
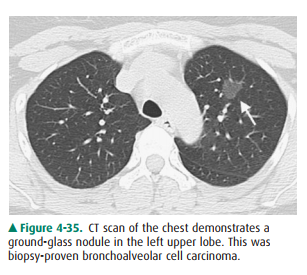
Non-small-cell bronchogenic carcinoma includes adeno-carcinoma, squamous-cell carcinoma, and large-cell carci-noma. Adenocarcinoma, the most common cell type, typically appears as a solitary pulmonary nodule in the pe-riphery of the lung. Bronchioalveolar cell carcinoma is a sub-type of adenocarcinoma that may present either as lobar airspace disease (Figure 4-39 A) or as diffuse, ill-defined pul-monary nodules (Figure 4-39 B). Bronchioalveolar cell carci-noma may also present as a solitary pulmonary nodule, usually a ground-glass nodule (see Figure 4-35). The second most common cell type, squamous-cell carcinoma, is associ-ated with cigarette smoking and most often is found as an en-dobronchial tumor resulting in lobar collapse (Figures 4-13 and 4-18). The endobronchial tumor is visible bronchoscop-ically, and sputum cytology may be diagnostic in this tumor. Squamous-cell carcinoma can also appear radiographically as a solitary cavitary mass (Figure 4-39 C) or noncavitary mass. Large-cell carcinoma is the least frequent cell type. Its appearance is that of a bulky lesion within the lung.
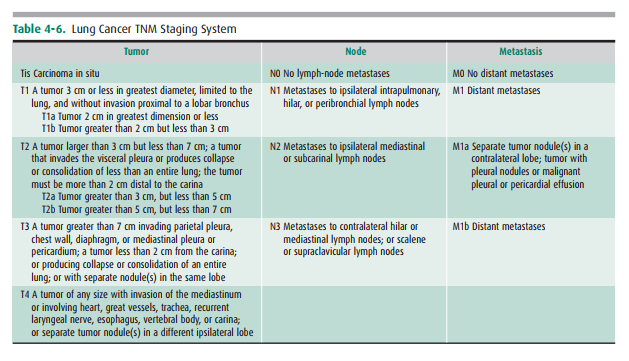
When non-small-cell lung cancer is diagnosed, the pa-tient undergoes a series of clinical and radiologic studies to determine the stage of the tumor. In the TNM staging sys-tem (Table 4-6), the categories of disease are stage IA, IB, IIA, IIB, IIIA, IIIB, or IV (Table 4-7). Stages I, II, and IIIA are surgically resectable. Patients with either stage IIIB or stage IV disease are not surgical candidates, but are treated with chemotherapy, radiation therapy, or both. In addition to helping define which treatment the patient should re-ceive, the stage of the tumor helps provide prognosis. Pa-tients with stage I disease have a 56% 5-year relative survival rate. Patients with stage IV disease have a 2% 5-year survival rate.

Related Topics