Chapter: Basic Radiology : Radiology of the Chest
Exercise: Airway Disease
EXERCISE 4-5.
AIRWAY DISEASE
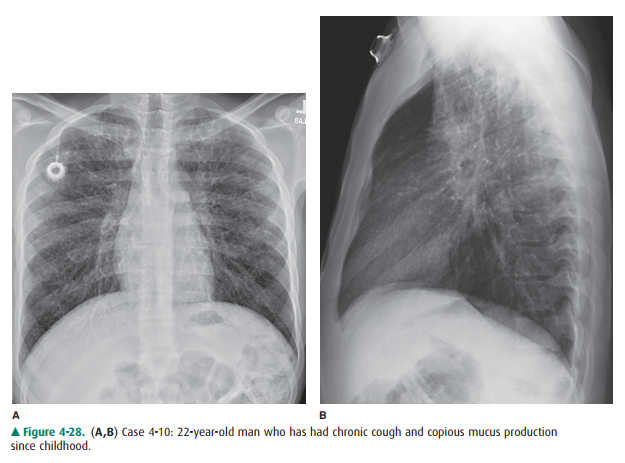
4-10. The most accurate
description of this chest radi-ograph (Figure 4-28 A,B) is
A.
decreased lung volume.
B.
diffuse thickening of the bronchial walls.
C.
cardiomegaly.
D.
pleural effusion.
E.
mediastinal shift.
Radiologic Findings
4-10. In this case, the
most prominent radiographic finding in Figure 4-28 A is coarse thickening of
the bron-chovascular bundles as they radiate from the hila. Thickened bronchial
walls may be identified as tram-track lines, which refers to the appearance of
the nearly parallel walls of bronchi oriented longitudinally. Care-ful
inspection shows that these are present throughout both lungs and are located
near the hila. Bronchial walls also project as ring-shaped opacities near the
hila whenthe bronchus is seen end-on. Both of these structures represent the
thick walls of dilated bronchi (bronchiec-tasis). The hila themselves are
slightly enlarged as a re-sult of a combination of enlarged hilar lymph nodes
and mild pulmonary arterial hypertension. The lung volume is increased. The
anterior clear space (retroster-nal area) is larger and more radiolucent than
normal. (B is the correct answer to Question 4-10).
Discussion
The cause of this patient’s
bronchiectasis is cystic fibrosis. The mucus in patients with cystic fibrosis
is thickened, and these patients do not have normal tracheobronchial
clear-ance. This abnormal clearance may cause mucoid impaction, and atelectasis
and pneumonia are frequent complications. Bronchiectasis can also occur as a
result of pneumonia in pa-tients without cystic fibrosis. In patients with
pneumonia, the bronchiectasis is more likely to be confined to a single lobe,
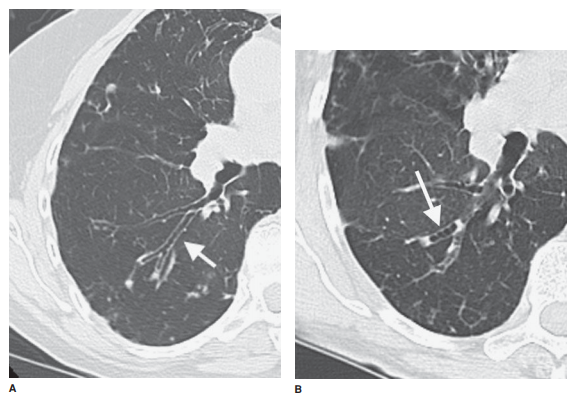
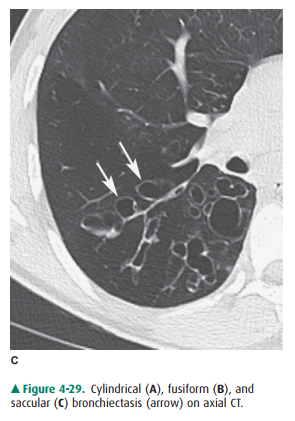
often a lower lobe. Bronchiectasis is divided into three groups: cylindrical,
fusiform (or varicose), and saccular (or cystic). These three groups not only
describe the appearance of the abnormal bronchi, but also give an indication as
to its severity. Cylindrical bronchiectasis (Figure 4-29 A), the mildest form,
is reversible and appears as thick-walled bronchi that fail to taper normally.
The more severe forms, fusiform and saccular, are irreversible. Fusiform
(Figure 4-29bronchiectasis has a beaded appearance, whereas the bronchi in
saccular (Figure 4-29 C) bronchiectasis end with clubbed, cystic areas. If the
severe forms are localized, surgi-cal resection may be curative. Medical
therapy with bron-chodilator and, when necessary, antibiotics is used when
surgery is not indicated.
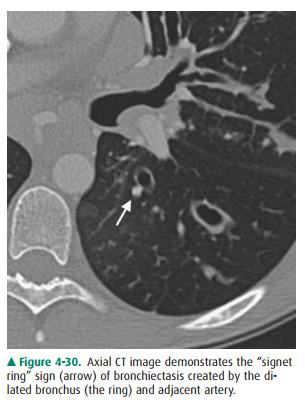
CT is the method of choice for
determining the presence and extent of bronchiectasis. When the bronchus is
perpen-dicular to the CT plane of section, bronchiectasis is identified as a
ring shadow adjacent to an opaque circle. The ring repre-sents the thickened
dilated bronchial walls. The opaque circle represents the pulmonary artery
adjacent to the dilated bronchus. This is called the “signet ring” sign (Figure
4-30). Bronchi and arteries travel together throughout the lung and are
normally of the same caliber.
Related Topics