Chapter: Clinical Anesthesiology: Perioperative & Critical Care Medicine: Critical Care
Ambient Oxygen Therapy Equipment: Variable-Performance Equipment
Variable-Performance
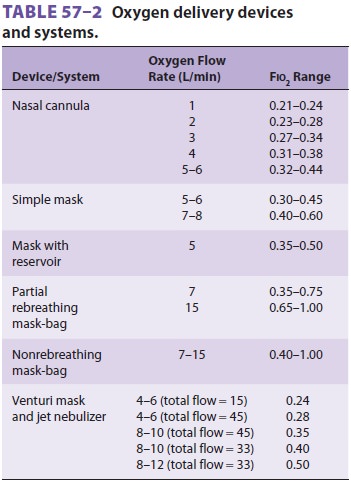
Equipment (Table 57–2)
Nasal Cannulas
The nasal cannula is available as
either a blind-ended soft plastic tube with an over-the-ear head-elastic or
dual-flow with under-the-chin lariat adjustment. Sizes appropriate for adults,
children, and infants are available. Cannulas are connected to flowmeters with
small-bore tubing and can rapidly be placed on most patients. The tension of
attachment should be firm yet comfortable enough to avoid pressure sores on the
ears, cheeks, and nose. Patients receiving long-term oxygen therapy most
commonly use a nasal cannula. The appliance is usually well tolerated, allowing
unen-cumbered speech, eating, and drinking. Cannulas can be combined with
spectacle frames for convenience or to improve acceptance by improving
cosmesis. Oxygen-conserving cannulas equipped with inlet res-ervoirs are
available for patients receiving long-term oxygen. Since oxygen flows
continuously, approxi-mately 80% of the gas is wasted during expiration.
There are valved reservoir devices that
permit storage of incoming oxygen until inspiration occurs.
The actual Fio2 delivered to adults with nasal cannulas is determined by oxygen flow,
nasopharyn-geal volume, and the patient’s inspiratory flow (which depends both
on Vt and inspiratory time). Oxygen from the cannula can fill the nasopharynx
after exha-lation, yet with inspiration, oxygen and entrained air are drawn
into the trachea. The inspired percent oxy-gen increases by approximately 1–2%
(above 21%) per liter of oxygen flow with quiet breathing in adults. Cannulas
can be expected to provide inspired oxygen concentrations up to 30–35% with
normal breathing and oxygen flows of 3–4 L/min. However, levels of 40–50% can
be attained with oxygen flows of greater than 10 L/min for short periods. Flows
greater than 5 L/min are poorly tolerated because of the discom-fort of gas
jetting into the nasal cavity and because of drying and crusting of the nasal
mucosa.
Data from “normal-breathing subjects” may not be accurate for acutely
ill tachypneic patients. Increasing Vt and reducing inspiratory time will
dilute the small flow of oxygen. Different propor-tions of mouth-only versus
nose-only breathing and varied inspiratory flow can alter Fio2 by up to
40%. In clinical practice, flow should be titrated accord-ing to vital signs,
pulse oximetry, and arterial blood gas measurements. Some patients with COPD
tend to hypoventilate with even modest oxygen flows, yet are hypoxemic on room
air. They may do well with cannula flows of less than 1–2 L/min.
Pediatric-sized nasal cannulas are available.
Special cannulas allow babies to nurse and produce less trauma of the face and
nose than oxygen masks. Because of the inherently reduced minute ventilation of
infants, flow requirements to the cannula must be proportionately reduced. This
generally requires a pressure-compensated flowmeter accurate at deliv-ering
oxygen flows in the less than 1–3 L/min range. Hypopharyngeal oxygen sampling
from infants breathing with cannulas has demonstrated mean Fio2 of 0.35, 0.45, 0.6, and 0.68 with flows of
0.25, 0.5, 0.75, and 1.0 L/min, respectively
Nasal Mask
The nasal mask is a hybrid of the nasal
cannula and a face mask. It can be applied to the face by either an
over-the-ear lariat or a headband strap. The lower edge of the mask’s flanges rests
on the upper lip, surrounding the external nose. Nasal masks have been shown to
provide supplemental oxygen equivalent to the nasal cannula under low-flow
conditions for adult patients. The primary advan-tage of the nasal mask over
nasal cannulas appears to be patient comfort. The nasal mask does not pro-duce
sores around the external nares and dry oxy-gen is not “jetted” into the nasal
cavity. The nasal mask should be considered if it improves patient comfort and
compliance.
“Simple” Oxygen Mask
The “simple” or oxygen mask is a disposable light-weight plastic device
that covers both nose and mouth. It has no reservoir bag. Masks are fastened to
the patient’s face by adjustment of an elastic headband; some manufacturers
provide a mal-leable metal nose-bridge adjustment device. The seal is rarely
complete: usually there is “inboard” leaking. Thus, patients receive a mixture
of oxygen and secondarily entrained room air. This varies depending on the size
of the leak, oxygen flow, and breathing pattern. Some brands of the simple mask
connect tubing to a standard tapered fitting; oth-ers have a small room
air–entrainment hole at the connection.
The body of the mask functions as a reservoir for both oxygen and
expired carbon dioxide. A minimum oxygen flow of approximately 5 L/min is
applied to the mask to limit rebreathing and the resulting increased
respiratory work. Wearing any mask appliance for long periods of time is uncom-fortable.
Speech is muffled and drinking and eating are difficult.
It is difficult to predict delivered Fio2 at specific oxygen flow rates.
During normal breathing, it is reasonable to expect an Fio2 of
0.3–0.6 with flows of 5–10 L/min, respectively. Oxygen levels can be increased
with smaller VT or slower breathing rates. With higher flows and ideal
conditions, Fio2 may approach 0.7 or 0.8.Masks lacking oxygen
reservoirs may be best suited for patients who require concentrations of oxygen
greater than cannulas provide, yet need oxy-gen therapy for fairly short
periods of time. Examples would include medical transport or therapy in the
postanesthesia care unit or emergency department. It is not the device of
choice for patients with severe respiratory disease who are profoundly
hypoxemic, tachypneic, or unable to protect their airway from aspiration.
Masks with Gas Reservoirs
Incorporating a gas reservoir is a logical adaptation to the simple
mask. Two types of reservoir mask are commonly used: the partial rebreathing
mask and the nonrebreathing mask. Both are dispos-able, lightweight,
transparent plastic under-the-chin reservoirs. The difference between the two
relates to use of valves on the mask and between the mask and the bag
reservoir. Mask reservoirs commonly hold approximately 600 mL or less of gas
volume. The phrase “partial rebreather” is used because “part” of the patient’s
expired VT refills the bag. Usually that gas is largely dead space that should
not result in significant rebreathing of car-bon dioxide.
The nonrebreather uses the same basic system
as the partial rebreather but incorporates flap-type valves between the bag and
mask and on at least one of the mask’s exhalation ports. Inboard leaking is
common, and room air will enter during brisk inspi-ratory flows, even when the
bag contains gas. The lack of a complete facial seal and a relatively small
reservoir influence the delivered oxygen concentra-tion. The key factor in
successful application of the masks is to use a sufficiently high flow of
oxygen, so that the reservoir bag is at least partially full during
inspiration. Typical minimum flows of oxygen are 10–15 L/min. Well-fitting
partial rebreathing masks provide a range of FIO2 from 0.35 to 0.60 with oxygen flows up to 10 L/min. With inlet flows of
15 L/min or more and ideal breathing conditions, FIO2 may approach 1.0. Either style of mask is
indicated for patients suspected of having significant hypoxemia, with
relatively normal spontaneous minute ventila-tion. Such patients may include
victims of trauma, myocardial infarction, or carbon monoxide expo-sure.
Profoundly dyspneic patients with gasping respiration may be served by a
fixed-performance, high-flow oxygen system.
Related Topics