Chapter: Medical Surgical Nursing: Respiratory Care Modalities
Weaning the Patient From the Ventilator
WEANING THE PATIENT FROM THE VENTILATOR
Respiratory weaning,
the process of withdrawing the patientfrom dependence on the ventilator, takes
place in three stages: the patient is gradually removed from the ventilator,
then from the tube, and finally from oxygen. Weaning from mechanical venti-lation
is performed at the earliest possible time consistent with patient safety. The
decision must be made from a physiologic rather than from a mechanical
viewpoint. A thorough under-standing of the patient’s clinical status is
required in making this decision. Weaning is started when the patient is
recovering from the acute stage of medical and surgical problems and when the
cause of respiratory failure is sufficiently reversed.
Successful
weaning involves collaboration among the physi-cian, respiratory therapist, and
nurse. Each health care provider must understand the scope and function of
other team members in relation to patient weaning to conserve the patient’s
strength, use resources efficiently, and maximize successful outcomes.
Criteria for Weaning
Careful
assessment is required to determine whether the patient is ready to be removed
from mechanical ventilation. If the patient is stable and showing signs of
improvement or reversal of the dis-ease or condition that caused the need for
mechanical ventilation, weaning indices should be assessed. These indices
include:
·
Vital capacity: the amount of air
expired after maximum in-spiration. Used to assess the patient’s ability to
take deep breaths. Vital capacity should be 10 to 15 mL/kg to meet the criteria
for weaning.
·
Maximum inspiratory pressure (MIP):
used to assess the pa-tient’s respiratory muscle strength. It is also known as
nega-tive inspiratory pressure and should be at least −20
cm H2O.
·
Tidal volume: volume of air that is
inhaled or exhaled from the lungs during an effortless breath. It is normally 7
to 9 mL/kg.
·
Minute ventilation: equal to the
respiratory rate multiplied by tidal volume. Normal is about 6 L/min.
·
Rapid/shallow breathing index: used
to assess the breathing pattern and is calculated by dividing the respiratory
rate by tidal volume. Patients with indices below 100 breaths/min/L are more
likely to be successful at weaning.
Other
measurements used to assess readiness for weaning include a PaO2
of greater than 60 mm Hg with an FiO2
of less than 40%. Stable vital signs and arterial blood gases are also
important pre-dictors of successful weaning. Once readiness has been
determined, the nurse records baseline measurements of weaning indices to
monitor progress (Cull & Inwood, 1999).
Patient Preparation
To
maximize the chances of success of weaning, the nurse must consider the patient
as a whole, taking into account factors that impair the delivery of oxygen and
elimination of carbon dioxide as well as those that increase oxygen demand
(sepsis, seizures, thy-roid imbalances) or decrease the patient’s overall
strength (nutri-tion, neuromuscular disease). Adequate psychological
preparation is necessary before and during the weaning process. Patients need
to know what is expected of them during the procedure. They are often
frightened by having to breathe on their own again and need reassurance that
they are improving and are well enough to handle spontaneous breathing. The
nurse explains what will hap-pen during weaning and what role the patient will
play in the pro-cedure. The nurse emphasizes that someone will be with or near
the patient at all times, and answers any questions simply and concisely.
Proper preparation of the patient can reduce the wean-ing time.
Methods of Weaning
Considerable
effort has been devoted to finding the best method of weaning from mechanical
ventilation, but research has not es-tablished which method is best (Tasota
& Dobbin, 2000). Suc-cess depends on the combination of adequate patient
preparation, available equipment, and an interdisciplinary approach to solv-ing
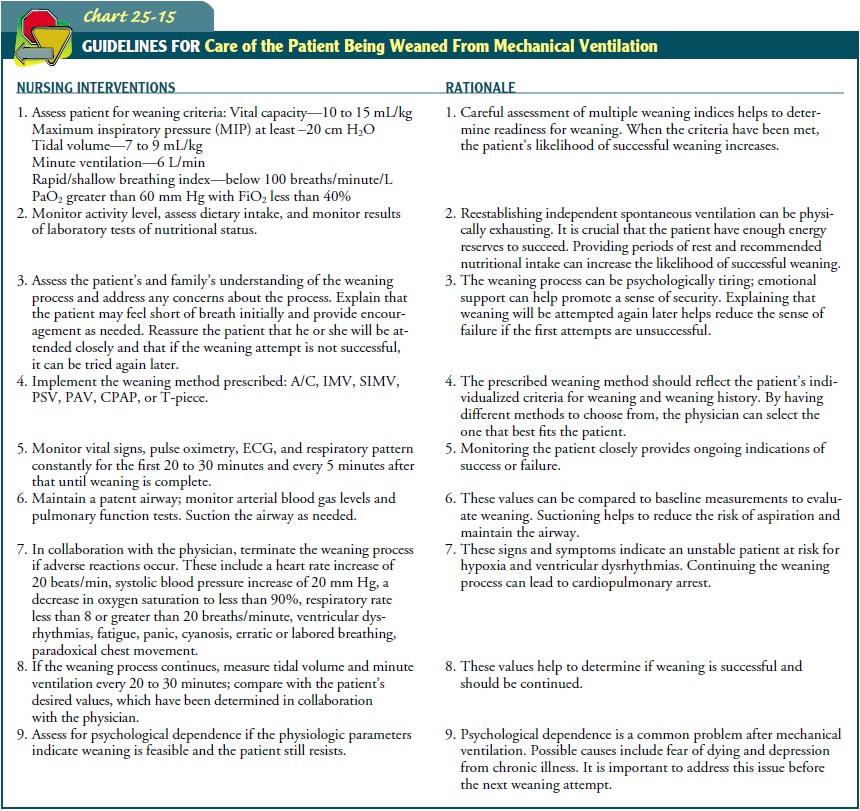
patient problems (Chart 25-15). The most common weaning methods in use today
are described below.
Assist–control
may be used as the resting mode for patients undergoing weaning trials. This
mode provides full ventilatory support by delivering a preset tidal volume and
respiratory rate; if the patient takes a breath, the ventilator delivers the
preset vol-ume. The cycle does not adapt to the patient’s spontaneous ef-forts.
The nurse assesses patients being weaned on this mode for the following signs
of distress: rapid shallow breathing, use of ac-cessory muscles, reduced level
of consciousness, increase in carbon dioxide levels, decrease in oxygen
saturations, and tachycardia.
The patient on intermittent mandatory ventilation (IMV) can increase the respiratory rate, but each spontaneous breath receives only the tidal volume the patient generates. Mechanical breaths are delivered at preset intervals and a preselected tidal volume, re-gardless of the patient’s efforts. IMV allows patients to use their own muscles of ventilation to help prevent muscle atrophy. IMV lowers mean airway pressure, which can assist in preventing baro-trauma.
Synchronized
intermittent mandatory ventilation (SIMV) de-livers a preset tidal volume and
number of breaths per minute. Between ventilator-delivered breaths, the patient
can breathe spontaneously with no assistance from the ventilator on those extra
breaths. As the patient’s ability to breathe spontaneously in-creases, the
preset number of ventilator breaths is decreased and the patient does more of
the work of breathing. SIMV is indi-cated if the patient satisfies all the
criteria for weaning but cannot sustain adequate spontaneous ventilation for
long periods.
IMV
and SIMV can be used to provide full or partial ventila-tory support. Nursing
interventions for both of these include monitoring progress by recording respiratory
rate, minute vol-ume, spontaneous and machine-generated tidal volume, FiO2,
and arterial blood gas levels.
The
pressure support ventilation (PSV)
mode assists SIMV by applying a pressure plateau to the airway throughout the
patient-triggered inspiration to decrease resistance by the tracheal tube and
ventilator tubing. Pressure support is reduced gradually as the patient’s
strength increases. A SIMV backup rate may be added for extra support. The
nurse must closely observe the patient’s respiratory rate and tidal volumes on
initiation of PSV. It may be necessary to adjust the pressure support to avoid
tachypnea or large tidal volumes.
The
proportional assist ventilation (PAV) mode of partial ven-tilatory support
allows the ventilator to generate pressure in pro-portion to the patient’s
efforts. With every breath, the ventilator synchronizes with the patient’s
ventilatory efforts (Giannouli,Webster, Roberts & Younes, 1999). Nursing
assessment should include careful monitoring of the patient’s respiratory rate,
arte-rial blood gases, tidal volume, minute ventilation, and breathing pattern.
The
continuous positive airway pressure (CPAP) mode allows the patient to breathe
spontaneously, while applying positive pressure throughout the respiratory
cycle to keep the alveoli open and promote oxygenation. Providing CPAP during
spontaneous breathing also offers the advantage of an alarm system and may
reduce patient anxiety if the patient has been taught that the ma-chine is
keeping track of breathing. It also maintains lung vol-umes and improves the
patient’s oxygenation status. CPAP is often used in conjunction with PSV.
Nurses should carefully as-sess for tachypnea, tachycardia, reduced tidal
volumes, decreas-ing oxygen saturations, and increasing carbon dioxide levels.
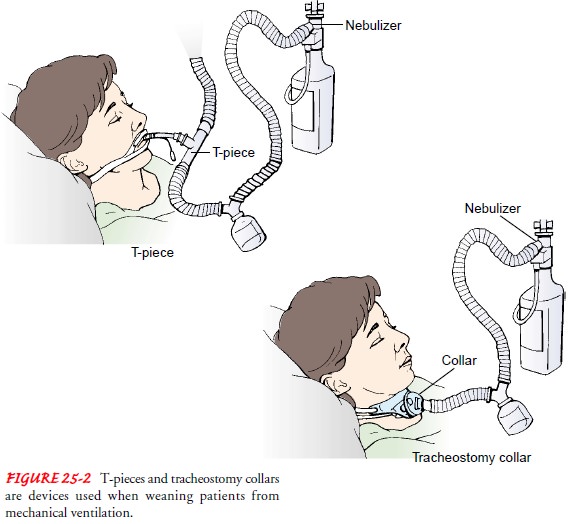
Weaning
trials using a T-piece or tracheostomy mask (see Fig. 25-2) are normally
conducted with the patient disconnected from the ventilator, receiving
humidified oxygen only, and performing all work of breathing. Patients who do
not have to overcome the resistance of the ventilator may find this mode more
comfortable, or they may become anxious as they breathe with no support from
the ventilator. During T-piece trials, the nurse monitors the pa-tient closely
and provides encouragement. This method of wean-ing is usually used when the
patient is awake and alert, is breathing without difficulty, has good gag and
cough reflexes, and is hemo-dynamically stable. During the weaning process, the
patient is maintained on the same or a higher oxygen concentration than when on
the ventilator. While on the T-piece, the patient should be observed for signs
and symptoms of hypoxia, increasing respi-ratory muscle fatigue, or systemic
fatigue. These include restless-ness, increased respiratory rate greater than
35 breaths/min, use of accessory muscles, tachycardia with premature
ventricular con-tractions, and paradoxical chest movement (asynchronous
breath-ing, chest contraction during inspiration and expansion during
expiration). Fatigue or exhaustion is initially manifested by an in-creased
respiratory rate associated with a gradual reduction in tidal volume; later
there is a slowing of the respiratory rate.
If
the patient appears to be tolerating the T-piece trial, a sec-ond set of
arterial blood gas measurements is drawn 20 minutes after the patient has been
on spontaneous ventilation at a con-stant FiO2
pressure support ventilation. (Alveolar–arterial equili-bration takes 15 to 20
minutes to occur.)
Signs
of exhaustion and hypoxia correlated with deterioration in the blood gas
measurements indicate the need for ventilatory support. The patient is placed
back on the ventilator each time signs of fatigue or deterioration develop.
If
clinically stable, the patient usually can be extubated within 2 or 3 hours of
weaning and allowed spontaneous ventilation by means of a mask with humidified
oxygen. Patients who have had prolonged ventilatory assistance usually require
more gradual weaning; it may take days or even weeks. They are weaned
pri-marily during the day and placed back on the ventilator at night to rest.
Because
patients respond in different manners to the various weaning methods, there is
no definitive way to assess which method is best. With all of the methods,
ongoing assessment of res-piratory status is essential to monitor patient
progress (Woodruff, 1999).
Successful
weaning from the ventilator is supplemented by in-tensive pulmonary care. The
following are continued:
·
Oxygen therapy
·
Arterial blood gas evaluation
·
Pulse oximetry
·
Bronchodilator therapy
·
Chest physiotherapy
·
Adequate nutrition, hydration, and
humidification
·
Incentive spirometry
These
patients still have borderline pulmonary function and need vigorous supportive
therapy before their respiratory status returns to a level that supports
activities of daily living.
Weaning From the Tube
Weaning
from the tube is considered when the patient can breathe spontaneously,
maintain an adequate airway by effectively cough-ing up secretions, swallow,
and move the jaw. If frequent suc-tioning is needed to clear secretions, tube
weaning may be unsuccessful (Ecklund, 1999). Secretion clearance and aspiration
risks are assessed to determine if active pharyngeal and laryngeal reflexes are
intact.
Once
the patient can clear secretions adequately, a trial period of mouth breathing
or nose breathing is conducted. This can be accomplished by several methods.
The first method requires changing to a smaller size tube to increase the
resistance to airflow and simultaneously plugging the tracheostomy tube (deflating
the cuff ). The smaller tube is sometimes replaced by a cuffless tra-cheostomy
tube, which allows the tube to be plugged at length-ening intervals to monitor
patient progress. A second method involves changing to a fenestrated tube (a
tube with an opening or window in its bend). This permits air to flow around
and through the tube to the upper airway and enables talking. A third method
involves switching to a smaller tracheostomy button (stoma button). A
tracheostomy button is a plastic tube approx-imately 1 inch long that helps to
keep the windpipe open after the larger tracheostomy tube has been removed.
Finally, when the patient demonstrates the ability to maintain a patent airway
with-out a tracheostomy tube, the tube can be removed. An occlusive dressing is
placed over the stoma, which usually heals anywhere from several days to many
weeks (Ecklund, 1999).
Weaning From Oxygen
The
patient who has been successfully weaned from the ventila-tor, cuff, and tube
and has adequate respiratory function is then weaned from oxygen. The FiO2
is gradually reduced until the PaO2
is in the range of 70 to 100 mm Hg while the patient is breathing room air. If
the PaO2 is less than 70 mm Hg on room air,
supplemental oxygen is recommended. The Centers for Medicare and Medicaid
Services, formerly the Health Care Fi-nancing Administration (HCFA), requires
that the patient’s PaO2 on room
air be less than 55 mm Hg for the patient to be eligible for financial
reimbursement for in-home oxygen.
Nutrition
Success
in weaning the long-term ventilator-dependent patient requires early and
aggressive but judicious nutritional support. The respiratory muscles
(diaphragm and especially intercostals) become weak or atrophied after just a
few days of mechanical ven-tilation, especially if nutrition is inadequate. Fat
kilocalories pro-duce less carbon dioxide than carbohydrate kilocalories. For
this reason, a high-fat diet may assist patients with respiratory failure who
are being weaned from mechanical ventilation. Research is being conducted on
the role of fatty acids in lung disease (Schwartz,2000). A high-fat diet may
provide as much as 50% of the total daily kilocalories. Adequate protein intake
is important in in-creasing respiratory muscle strength. Protein intake should be
ap-proximately 25% of total daily kilocalories, or 1.2 to 1.5 g/kg/day. Because
a high-carbohydrate diet can lead to increased carbon diox-ide production and
retention, total carbohydrate intake should not exceed 25% of total daily
kilocalories, or 2 g/kg/day in pa-tients being weaned from mechanical
ventilation. Care must be taken not to overfeed patients because excessive
intake can raise the demand for oxygen and the production of carbon dioxide.
Total daily kilocalories should be closely monitored (Lutz & Prytulski,
2001).
Soon
after the patient is admitted, a consultation with a di-etitian or nutrition
support team should be arranged to plan the best form of nutritional
replacement. Adequate nutrition may de-crease the duration of mechanical
ventilation and prevent other complications, especially sepsis. Sepsis can
occur if bacteria enter the bloodstream and release toxins that, in turn, cause
vasodila-tion and hypotension, fever, tachycardia, increased respiratory rate,
and coma. Aggressive treatment of sepsis is essential to re-verse this threat
to survival and to promote weaning from the ven-tilator when the patient’s
condition improves. Optimal nutritional intake is an essential part of the
treatment of sepsis.
Related Topics