Chapter: Medical Surgical Nursing: Respiratory Care Modalities
Problems With Mechanical Ventilation
PROBLEMS WITH MECHANICAL VENTILATION
Because
of the seriousness of the patient’s condition and the highly complex and
technical nature of mechanical ventilation, a num-ber of problems or
complications can occur. Such situations fall into two categories: ventilator
problems and patient problems. In either case, the patient must be supported
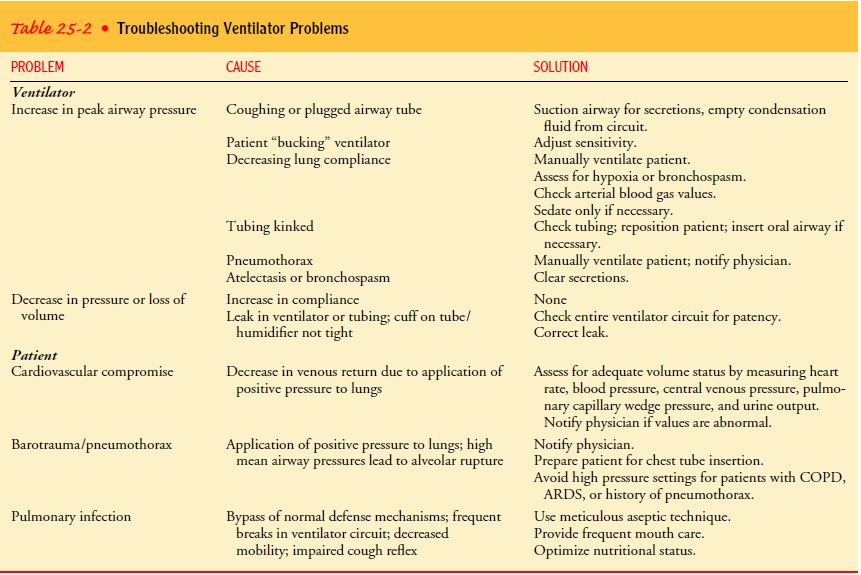
while the problem is identified and corrected. Ventilator complications include
cardio-vascular compromise, pneumothorax, and pulmonary infection. These
problems, their probable causes, and solutions are listed in Table 25-2.
BUCKING THE VENTILATOR
The
patient is “in sync” with the ventilator when thoracic ex-pansion coincides
with the inspiratory phase of the machine and exhalation occurs passively. The
patient is said to fight or buck the ventilator when out of phase with the
machine. This is man-ifested when the patient attempts to breathe out during
the ven-tilator’s mechanical inspiratory phase or when there is jerky and
increased abdominal muscle effort. The following factors con-tribute to this
problem: anxiety, hypoxia, increased secretions, hypercapnia, inadequate minute
volume, and pulmonary edema. These problems must be corrected before resorting
to the use of paralyzing agents to reduce bucking; otherwise, the underlying
problem is simply masked and the patient’s condition will con-tinue to
deteriorate.
Muscle
relaxants, tranquilizers, analgesic agents, and paralyz-ing agents are
sometimes administered to patients receiving me-chanical ventilation. Their
purpose is ultimately to increase the patient–machine synchrony by decreasing
the patient’s anxiety, hyperventilation, or excessive muscle activity. The
selection and dose of the appropriate medication are determined carefully and
are based on the patient’s requirements and the cause of his or her
restlessness. Paralyzing agents are always used as a last resort, and always in
conjunction with a sedative medication.
Nursing Management
PROMOTING HOME AND COMMUNITY-BASED CARE
Increasingly, patients are being cared for in extended care
facilities or at home while on mechanical ventilators, with tracheostomy tubes,
or on oxygen therapy. Patients receiving home ventilator care usually have
chronic neuromuscular conditions or COPD.
Teaching Patients Self-Care.
Caring for the patient
with mechan-ical ventilator support at home can be accomplished successfully,
but the family must be emotionally, educationally, and physically able to
assume the role of primary caregiver. A home care team con-sisting of the
nurse, physician, respiratory therapist, social service or home care agency,
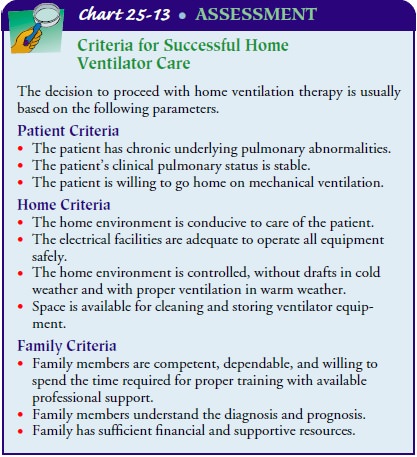
and equipment supplier is needed. The home is evaluated to determine if the electrical
equipment needed can be operated safely. A summary of the basic assessment
criteria needed for successful home care is presented in Chart 25-13.
Once the decision is made to
initiate mechanical ventilation at home, the nurse prepares the patient and
family for home care. It is important to teach them about the ventilator,
suctioning, tra-cheostomy care, signs of pulmonary infection, cuff inflation
and deflation, and assessment of vital signs. Teaching often begins in the
hospital and continues at home. Nursing responsibilities in-clude evaluating
the patient’s and family’s understanding of the information presented.
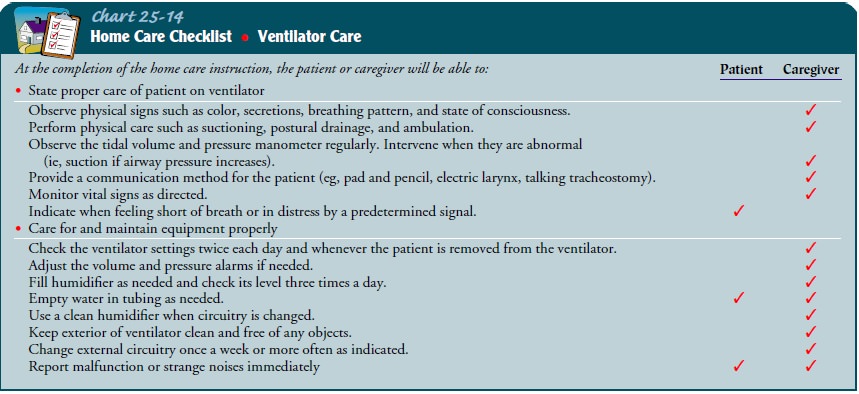
The nurse teaches the family cardiopulmonary resuscitation, including mouth-to-tracheostomy tube (instead of mouth-to-mouth) breathing. The nurse also explains how to handle a power failure, which usually involves converting the ventilator from an electrical power source to a battery power source. Conversion is automatic in most types of home ventilators and lasts approxi-mately 1 hour. The nurse instructs the family on using a manual self-inflation bag should it be necessary. Some of the patient’s and family’s responsibilities are listed in Chart 25-14.
Continuing Care.
A
home care nurse monitors and evaluates howwell the patient and family are
adapting to providing care in the home. The nurse also assesses the adequacy of
ventilation and oxygenation as well as airway patency. The nurse addresses any
unique adaptation problems the patient may have and listens to the patient’s
and family’s anxieties and frustrations, offering sup-port and encouragement
where possible. The home care nurse helps identify and contact community
resources that may assist in home management of the patient with mechanical
ventilation.
The
technical aspects of the ventilator are managed by vendor follow-up. A
respiratory therapist usually is assigned to the pa-tient and makes frequent
home visits to evaluate the patient and perform a maintenance check of the
ventilator.
Transportation
services are identified should the patient re-quire transportation in an
emergency. These arrangements must be made before an emergency arises.
Providing the opportunity for ventilator-dependent patients to return home to live with their families in familiar surround-ings can be a positive experience. The ultimate goal of home ven-tilator therapy is to enhance the patient’s quality of life, not simply to support or prolong life.
Related Topics