Chapter: Medicine and surgery: Haematology and clinical Immunology
Transfusion medicine
Transfusion medicine
Transfusion medicine
Blood grouping
Grouping is the process by which the patient’s ABO and rhesus D status are determined. The patient’s blood sample is separated into cells and serum. These are grouped separately in order to act as a double check.
· The patient’s red cells are incubated with commercial antibody preparations against the A, B and D antigens. By examining the pattern of agglutination the blood group can be determined.
· The patients serum is incubated with red cells of known blood group (A, B, AB and O Rh+ ) and the agglutination patterns are read to check the blood group.
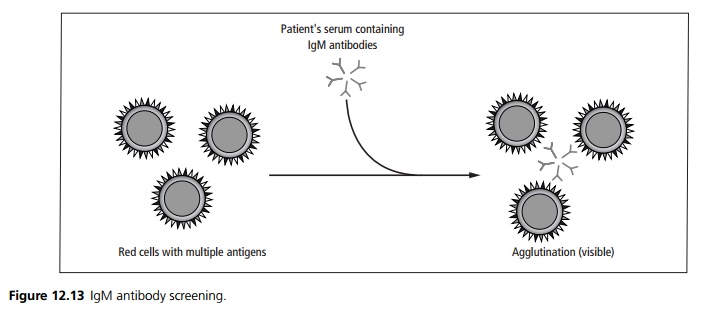
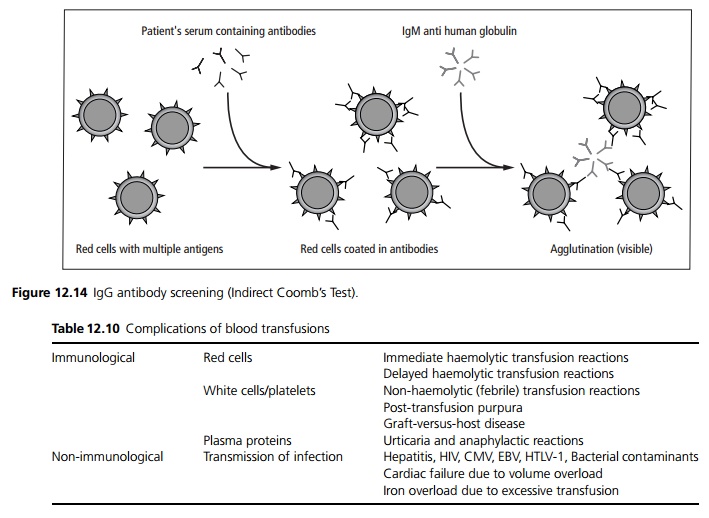
Antibody screening
The patient’s serum is also tested for atypical red cell antibodies using at least two Group O donors who express a wide range of antigens. Any IgM antibodies present will automatically agglutinate the donor red cells suspended in saline (see Fig. 12.13). IgG antibodies are detected by the indirect Coomb’s test (see Fig 12.14).
Cross matching
A group matched blood unit (antigen matched if patient has atypical antibodies) is cross matched with the patient’s serum. A full cross match consists of incubating the patient’s serum with the donor red cells and then performing a direct agglutination and indirect Coomb’s test as above. In an emergency, if the patient has no atypical antibodies a rapid cross match can be performed by briefly incubating the patient’s serum with the donor cells and examining for agglutination.
Transfusion complications
Complications to blood transfusions can be divided into immunological complications and other problems (see Table 12.10).
Immediate haemolytic transfusion reaction is the most serious and is usually due to ABO incompatibility. There is intravascular haemolysis and coagulation. Patients become acutely unwell and shocked within a few minutes of commencing the transfusion.
Delayed haemolytic reactions occur in patients previously sensitised to minor blood group antigens (eg Duffy, Kell, Kidd) by previous transfusion or pregnancy. Patient may develop anaemia and jaundice about a week after the transfusion.
Urticarial transfusion reactions are of unknown aetiology but possibly result from antibodies reacting with plasma proteins in the transfusion. The transfusion should be slowed or stopped and an antihistamine given (e.g. chlorpheniramine).
Non-haemolytic or febrile transfusion reactions are due to the presence of antibodies to leucocytes in the transfusion. Patients typically develop flushing, tachycardia, fever and rigors towards the end of transfusion.
Anaphylactic transfusion reactions can occur in IgA deficient individuals (1 in 600 individuals) mediated by histamine and other vasoactive mediators (see below). Patients develop vasodilation, hypotension, bronchoconstriction and laryngeal constriction. It is treated as for anaphylaxis. Any future transfusions should be with washed red cells, autologous blood or blood from IgA deficient donors.
If a transfusion reaction is suspected any ongoing transfusion should be stopped. The remaining blood unit and a sample of the patient’s blood should be sent to the laboratory for repeat cross match. Other supportive treatments may be required.
Problems of massive transfusion
Transfusion equivalent to replacing the entire circulating volume within a 24 hour period is defined as a massive transfusion. This may be required following trauma, gastrointestinal or obstetric haemorrhage.
Thrombocytopenia may result from the underlying bleeding and because there are no platelets in packed red cells. In severe cases platelet transfusion may also be required.
Coagulation factor deficiency results from the dilution effect of massive fluid transfusion as there is a lack of factors in packed red cells. There may also be a consumptive coagulopathy due to ongoing bleeding. Patients may require fresh frozen plasma and/or cryoprecipitate.
Hypocalcaemia results from the sodium citrate (which chelates calcium) used as an anti-coagulant in blood products. If the ECG shows a prolonged QT interval i.v. calcium gluconate is required.
Hyperkalaemia from degeneration of red cells within stored blood particularly if there is associated renal failure.
Hypothermia from infusion of cold blood may precipitate a cardiac arrest.
Acute respiratory distress syndrome may occur due to hypovolaemia, poor tissue perfusion or if patients are over-transfused.
Related Topics