Chapter: Medicine and surgery: Haematology and clinical Immunology
Glucose-6-phosphate dehydrogenase (G6PD) deficiency - Metabolic defects
Metabolic defects
Glucose-6-phosphate dehydrogenase (G6PD) deficiency
Definition
An X-linked genetic enzyme deficiency resulting in ab-normal metabolism within red cells and haemolysis.
Incidence
Affects 200 million people worldwide.
Age
Congenital
Sex
Males affected, females have 50% of cells affected.
Geography
More common in Africa, Mediterranean, Middle East and South East Asia.
Aetiology
The gene for G6PD is carried on the X chromosome. There are over 400 structural types of the G6PD gene, it can therefore be considered to be a polymorphism rather than a defect. Differing isoforms have differing activity. The incidence of abnormal genes in some countries is so high that females may have two X chromosomes each with an abnormal G6PD coded. Random X inactivation (Lyonisation) means that some heterozygous females may also have symptoms.
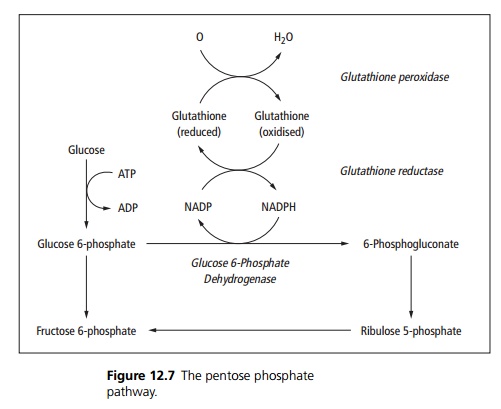
Pathophysiology
Normally red cells are protected from the action of free radicals by glutathione. The pentosephosphate pathway is used to keep glutathione in its reduced form. G6PD is one of the enzymes involved in the pentose phosphate pathway (see Fig. 12.7).
G6PD deficiency leads to haemolysis in times of high oxidative stress and results in
· Membrane oxidation and crosslinking of spectrin, which decreases flexibility and increases permeability of the red cell membrane.
· Oxidation of haemoglobin to methaemoglobin; the globin chains then precipitate as Heinz bodies, which are removed from the red cells in the spleen.
Clinical features
With such a wide variety of genes and enzymatic activity, a spectrum of clinical conditions occur. G6PD deficiency is a cause of prolonged neonatal jaundice. The WHO classifies G6PD deficiency into two categories:
Class I: Extremely low G6PD activity causing lifelong haemolytic anaemia.
Class II and III: No chronic haemolysis but susceptibility to haemolytic episodes at times of high oxidant stress such as with infections or drugs, e.g. primaquine, sulphonamides, nitrofurantoin, ciprofloxacin, dapsone and naphthalene (mothballs).
Favism is acute haemolysis following ingestion of fava (broad) beans.
Complications
After an oxidant shock the haemoglobin levels may fall dramatically with death following unless transfused.
Investigations
During an attack the blood film may show irregularly contracted cells, bite cells (indented membrane), blister cells (cells in which haemoglobin appears detached from the cell membrane), Heinz bodies and increased reticulocytes. Between attacks the G6PD level can be measured.
Management
Avoid causative drugs and foods, treat infections and transfuse as required.
Related Topics