Chapter: Basic & Clinical Pharmacology : Pharmacologic Management of Parkinsonism & Other Movement Disorders
Surgical Procedures - Parkinsonism
SURGICAL PROCEDURES
In patients with
advanced disease that is poorly responsive to pharmacotherapy, worthwhile
benefit may follow thalamotomy (for conspicuous tremor) or posteroventral
pallidotomy. Ablative surgical procedures, however, have generally been
replaced by functional, reversible lesions induced by high-frequency deep brain
stimulation, which has a lower morbidity.
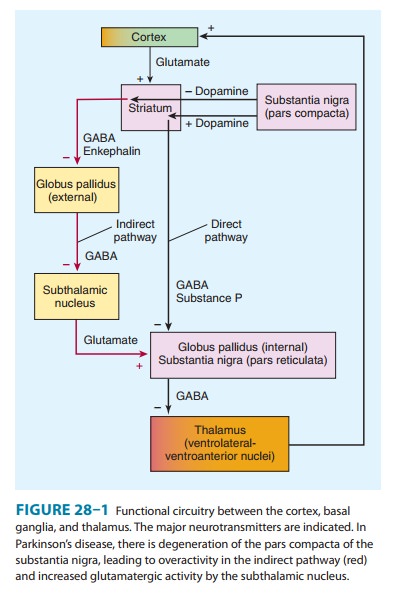
Stimulation of the
subthalamic nucleus or globus pallidus by an implanted electrode and stimulator
has yielded good results for the management of the clinical fluctuations
occurring in advanced parkinsonism. The anatomic substrate for such therapy is
indi-cated in Figure 28–1. Such procedures are contraindicated in patients with
secondary or atypical parkinsonism, dementia, or failure to respond to
dopaminergic medication.
In a controlled trial
of the transplantation of dopaminergic tis-sue (fetal substantia nigra tissue),
symptomatic benefit occurred in younger (less than 60 years old) but not older
parkinsonian patients. In another trial, benefits were inconsequential.
Furthermore, uncontrollable dyskinesias occurred in some patients in both
studies, perhaps from a relative excess of dopamine from continued fiber
outgrowth from the transplant. Additional basic studies are required before
further trials of cellular therapies—inparticular, stem cell therapies—are
undertaken, and such approaches therefore remain investigational.
Related Topics